Common Health Challenges
Download student handouts: Common Health Challenges handouts [Word doc].
Suggested Learning Strategies
Strategies that Focus on Caring
1. Contributing to a Broadened Understanding of Common Health Challenges
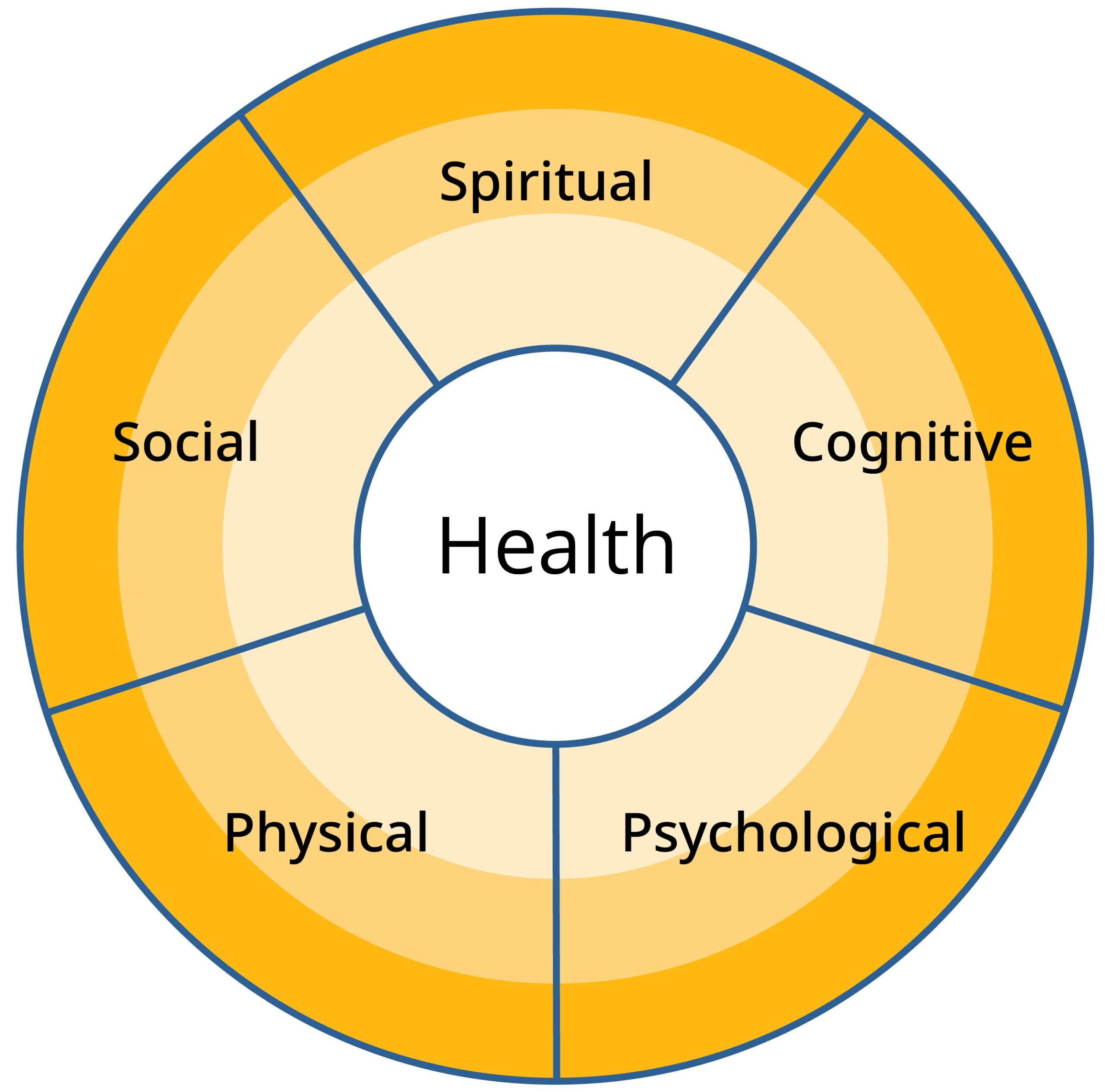
Using the health wheel below as a guide, invite students, working in small groups, to discuss how common health challenges might affect all areas of health and healing.
Each group may be assigned a specific health challenge and given the task of identifying the primary components of the health challenge (e.g., pain, loss of function, immobility, fatigue, confusion, stress).
With this information, the group will identify how these changes might affect all other aspects of the person’s health (e.g., how fatigue might affect psychological, cognitive, social, and spiritual health).
The group will then discuss how changes in each dimension of health might positively contribute to healing. Each group will report back to the whole class.
Note: The health wheel is first introduced in the Lifestyle and Choices course. See “The Health Wheel: Indicators of Health” for more information.
2. Contributing to Person-Centred Care
The above process could be undertaken using scenarios of real or fictitious individuals who are struggling with one or more of the common health challenges studied in this course. Ask students to work in small groups to discuss how the changes in health brought about by the health challenge(s) are affecting all dimensions of the person’s health and healing and how each level of needs (as described by Maslow) is affected. The group will then discuss how changes in each dimension of health might positively contribute to healing. Each group will report back to the whole class.
3. Unfolding Case Study: Caring for Peter Schultz
As a homework assignment, ask students to review relevant textbooks, online courses, or other course materials describing cerebral vascular accidents (CVAs).
- Whole Class Review and Discussion
- In class, review the risk factors, signs, and symptoms of CVAs. List them on the whiteboard for reference. Following this, have students read the account describing the CVA experienced by Peter Schultz. See STUDENT HANDOUT 1.
- Small Group Discussion
- Working in small groups, students should apply their knowledge about CVAs to the scenario below by responding to the following discussion questions:
- What signs and symptoms of CVA did Peter experience?
- What were the immediate and long-term results of the CVA experienced by Peter?
- Working in small groups, students should apply their knowledge about CVAs to the scenario below by responding to the following discussion questions:
- Whole Class Debrief
- Come back together as a class and summarize the findings of each group. Highlight any signs, symptoms, and results of CVA that were not identified.
Note: Students could be instructed to add the scenario and session materials to their client portfolio for Peter Schultz.
STUDENT HANDOUT 1
Unfolding Case Study: Caring for Peter Schultz
Cerebral Vascular Accidents (CVAs)
DIRECTIONS: Read the following account describing the CVA experienced by Peter Schultz. Working in small groups, apply your knowledge about CVAs to the scenario below by responding to the following discussion questions:
- What signs and symptoms of CVA did Peter experience?
- What were the immediate and long-term results of the CVA experienced by Peter?
What I thought was the beginning happened March 3, 1995, when Peter was 77 [years old]. I awoke in the night to hear Peter in the bathroom coughing and hacking as though to rip his throat out. He finally stumbled back to bed and went to sleep. I arose fairly early to prepare breakfast for his sister and her husband who had been visiting us and were leaving that morning for Alberta. We three were sitting at the table waiting for Peter who was slow making an appearance. When he did, we couldn’t understand a word he said as his speech was so confused. He didn’t seem to realize there was anything wrong. We struggled through breakfast trying to persuade him to see a doctor, but he insisted he simply had a little sore throat, so finally our guests left and we began our day.
Peter lay down on the couch and slept. Something was wrong, but I didn’t know what. Later I went to my daughter’s house to give the kids a piano lesson. When I told them what had happened, my son-in-law immediately phoned the doctor who said I must bring Peter into the office. I went home and did that.
“His blood pressure is out of sight,” the doctor said. “He’s had a stroke. I’ll arrange for a brain scan and we’ll see what the damage is.”
The scan showed that he had had several prior strokes that hadn’t been obvious. Medication for high blood pressure was prescribed, and I made sure Peter took his pills each day. I had no experience looking after someone who was sick, but Peter didn’t seem sick anyway, just a bit confused sometimes. However, as time went on, I began to notice some personality changes. He was often rude to me in front of friends, cried easily, and clung to me almost obsessively; table manners seemed to slip away and he was sometimes extremely impolite.
Metzger, Z.B. (2010). The Last Lap of the Long Run, Addendum to “On the Long Run”: An Account of our Travels with Dementia. This material is licensed under a CC BY-SA 4.0 licence.
4. Case Study: Creating a Caring Environment for a Patient Who is Dying
Share the following case study with students and use the discussion questions to guide a whole group discussion.
A 61-year-old male is being admitted to the unit by stretcher from Emergency. He was receiving palliative end-of-life care at home, but has been admitted due to a pain crisis. You enter the room with the RN from your unit, and under the direction of the RN, you assist in moving the patient from stretcher to bed. With a gentle touch and a caring smile, you introduce yourself.
As the RN gets the report, you continue to help position the patient. You go for more pillows to help with positioning, get a warm blanket, and retrieve other care items. You ask the RN how you can help (for example, find an IV pole, collect mouthwash supplies, or get ice water).
Once the patient is settled, you turn your attention to the family. You consider how many chairs they will need in the room and ask if you can get them something to drink. You also show them where the washroom, ice machine, and public telephone are located.
Remember to consider the family in planning the care of your patient. The death of a loved one is an experience that stays with most people forever. It is our job to be supportive during this time. The RN will need to pay attention to eliminating the pain crisis and attend to the other needs while you help to create a caring environment.
Questions for Discussion:
- Have you ever visited someone who was dying in the hospital?
- What did staff do to help make your loved one feel better?
- What could have been done differently that would have helped your loved one?
- How did staff help you during this time?
- What does empathy mean to you? How could you demonstrate empathy with the patient?
Note: This case study is used with permission from Island Health. (2012). Transitional Learning Continuum, Health Care Assistant in Acute Care Curriculum.
Strategies that Focus on Critical Thinking, Problem-Solving, and Decision-Making
1. Classroom Debate Activity
Invite students to engage in a debate about a topic discussed in this course. Divide the class into small groups of three to five students and assign two groups to each of the topics outlined; one group will take a pros position towards the topic and the other group will take a cons position.
Ask each group to identify two to three reasons to support the position they have been assigned. Then, with the instructor acting as the moderator, the two groups will engage in a debate using the following structure:
- Each group provides a brief introduction to their position on the topic.
- In alternating format, the two groups present the two or three reasons identified to support their position.
- Each group provides a brief closing statement.
After the debate, briefly come together as a larger group and summarize the positions presented. Invite feedback from the students not involved in the debate and discuss further considerations. Alternate groups until all students have participated in a debate.
Debate topics for Common Health Challenges.
- HCAs should assist clients to smoke (e.g., wheel them outside, light the cigarette, or prepare the vape cartridge).
- The family of an adolescent client with a developmental disability should be informed of the client’s involvement in a romantic or sexual relationship.
- Should families have the right to override a patient’s wishes regarding end-of-life care?
2. Developing a Best Practices Tool to Support a Client Who is Dying
Invite students, working alone or in small groups, to develop a tool (for example, a checklist of best practices) that would aid them when they are supporting a client who is dying.
Based on what they have learned about end-of-life care, what regular observations should be made:
- In respect to physical changes and comfort needs of the client?
- In respect to psychological and cognitive changes in the client?
- In respect to their social and spiritual health needs?
After developing the tool, students will discuss how the information will influence choices they will make about caregiving practice and how they will evaluate the care they provide.
3. Case Studies and Discussion: Trajectories of Illness and Dying
Using the resource The five trajectories: Supporting patients during serious illness from the California State University Shiley Institute for Palliative Care, introduce the concept of the trajectories of illness and dying to the class. Explain that this activity with involve:
- Exploring the five trajectories of illness and dying
- Identifying common health challenges that contribute to each trajectory
- Integrating a palliative care approach into each case study
- Begin the activity by listing the five trajectories on a whiteboard:
- Sudden death
- Terminal disease
- Major organ failure
- Frailty
- Catastrophic event
- Have the students read the description of the five sudden death trajectories in the resource. The trajectory descriptions are located after the “Case study” and before the subhead “Advance care planning.” At this point, the students should only read the trajectory description, not the case studies, care planning or key practice points.
- Divide the students into small groups to discuss the following:
- What are the differences between the five trajectories?
- What factors impact the prevalence, circumstances, and ways in which people die? (E.g., access to health care, quality of their diet, safety in work settings, advances in medicine, pollution and exposure to toxins, genetics, lifestyle)
- What information did you find surprising or interesting?
- Bring the students back together in a large group and ask for one student from each group to give a short summary of their discussion.
- As a large group, ask the students to identify common health challenges that contribute to each trajectory. Write these challenges on the whiteboard beside each trajectory. Examples are included below:
- Sudden death (e.g., fatal major heart attack or stroke, car accident, sudden acute illness)
- Terminal disease (e.g., cancer)
- Major organ failure (e.g., chronic obstructive pulmonary disease, congestive heart failure, renal disease)
- Frailty (e.g., dementia, multiple sclerosis, Parkinson’s disease, failure to thrive)
- Catastrophic event (e.g., hip fracture, non-fatal heart attack or stroke, traumatic brain injury, accident)
- Divide the students back into small groups. Students will read each of the five case studies in the resource (in the coloured text boxes on pages 2, 4, 6, 8, and 10) and then discuss the following:
- What impact would each trajectory of dying have on the patient, the family and the health care providers? For each person, consider the impact in terms of the dimensions of health.
- What is the role of advance care planning in improving care during each trajectory?
- How could a palliative care approach be integrated into the care of the patient and their families for each trajectory?
- How would different health care settings (e.g., complex care, home care, hospice, acute care) impact the palliative care approach?
References
Ballentine, J. M. (2018). The five trajectories. Supporting patients during serious illness. Shiley Institute for Palliative Care, California State University. https://csupalliativecare.org/wp-content/uploads/Five-Trajectories-eBook-02.21.2018.pdf
Milne Library. (2015). Types and variability within illness trajectories. https://milnepublishing.geneseo.edu/nursingcare/chapter/types-and-variability-within-illness-trajectories/#:~:text=with%20the%20loss.-,Terminal%20illness,or%20days%20before%20they%20die
4. Critical Thinking Activity: Responding to Clients with Common Health Challenges
Students will use their knowledge about communication, common health challenges, and observing and reporting to identify and respond to a variety of health-related situations.
Six scenarios of clients with common health challenges are provided below. Included for each scenario are an HCA role card, a client role card, and a client profile. The client profile should be used to inform client care; alternately, it could be used to populate preferred templates in use by the program (e.g., bedside care plan or assignment sheets). The material provided for this activity has been formatted in a way that will facilitate its direct use in the educational setting.
Students may enjoy practising this activity in the lab, with measures taken to simulate a real-life setting. This critical thinking activity could also be adapted for use during the Personal Care and Assistance course.
Depending on program sequencing, the scenarios and client profiles could be further adapted to increase the complexity of this activity. This could be accomplished by incorporating additional props or equipment or by adding information to the client profile (e.g., medication information).
While not directly indicated, the health-related situations are listed below for instructor reference. Students in the HCA role should be able to identify these situations (using observation and reporting) through the role play and when documenting. The instructor will highlight these during the debrief.
- Role Play 1: Responding to a client showing signs of hypoglycemia
- Role Play 2: Responding to a client showing signs of orthostatic hypotension
- Role Play 3: Responding to a client indicating she is hungry
- Role Play 4: Responding to a client showing signs of pneumonia
- Role Play 5: Responding to a client showing signs of a urinary tract infection
- Role Play 6: Responding to a client showing signs of constipation
Setting Up the Activity
A. Role Play
Have students work in pairs, with one acting as the client and the other as the HCA. Provide role-play cards in such a way that students do not see the card for the alternate role. The student acting as the client will read the client role card and follow the directions provided. The student acting as the HCA will read the HCA role card and then use critical thinking skills to respond to the situation they are presented with. The client profile for each role play can be provided to both students and/or given to them to share.
Students playing the HCA role should be reminded to respond to the scenario based on their observations, communication with the client, and the accompanying client profile (or assignment sheet and/or bedside care plan).
Students should be instructed to report any emergencies to the instructor, who could take on the role of the team leader.
Students should be directed to alternate roles after each role play and get new role cards from the instructor after completing required documentation (see B).
B. Documentation Exercise
After each role play is complete, ask the pairs to prepare a written report describing the situation. If desired, the instructor could request that a specific documentation format is followed, such as the one to be used in the practice education setting. At a minimum, the following should be documented:
- What the HCA observed, including symptoms the client reported to them
- What the HCA did
- When the HCA did it
- The client’s response, as observed by the HCA
C. Debrief
After students have completed this activity, convene as a class to review the common health challenges presented. Discuss appropriate response(s) and reporting for each scenario, highlighting which situations would require immediate reporting to the team leader.
ROLE PLAY CARDS
ROLE PLAY 1: HCA ROLE CARD
You are working for a home support agency. Today you are visiting Jenny Smith for the first time. Enter the home, greet your new client, and introduce yourself. Respond to the situation you are presented with.
ROLE PLAY 1: CLIENT ROLE CARD
Your name is Jenny Smith and you are 72 years old. After the HCA greets you, tell them you feel dizzy and sweaty and that you are hungry because you skipped breakfast today.
ROLE PLAY 2: HCA ROLE CARD
You are working in an assisted living residence. Today you will be escorting Ali Singh to the dining room for lunch. Enter her room, greet her, and introduce yourself. Respond to the situation you are presented with.
ROLE PLAY 2: CLIENT ROLE CARD
Your name is Ali Singh, and you are 88 years old. After the HCA provides introductions and checks your bedside care plan, they will ask you to walk to the dining room. As you get up from your chair, act dizzy. Sit down again and tell the HCA you feel dizzy.
ROLE PLAY 3: HCA ROLE CARD
You are working in a group home setting. Today you will be assisting Aiko Tanaka who has ataxic cerebral palsy. Enter her room, greet her, and introduce yourself. Respond to the situation you are presented with.
ROLE PLAY 3: CLIENT ROLE CARD
Your name is Aiko Tanaka, and you are 42 years old. You have ataxic cerebral palsy and are unable to speak. When the HCA arrives, use gestures to indicate that you are hungry.
ROLE PLAY 4: HCA ROLE CARD
You are working in an acute care setting. Today you will be providing care to Matika Tahoma who has had hip replacement surgery. Enter his room, greet him, and introduce yourself. Respond to the situation you are presented with.
ROLE PLAY 4: CLIENT ROLE CARD
Your name is Matika Tahoma. When the HCA enters your room, start coughing. Tell the HCA that you have chest pain and are feeling cold.
ROLE PLAY 5: HCA ROLE CARD
You are working in a complex care home. Today you will be assisting Gabriela Martinez with her breakfast. Enter her room and greet her. Respond to the situation you are presented with.
ROLE PLAY 5: CLIENT ROLE CARD
Your name is Gabriela Martinez. After the HCA greets you, act as if you are confused. Indicate that you have pain in your lower abdomen.
ROLE PLAY 6: HCA ROLE CARD
You are working in a complex care home. Today you will be assisting Erika Karlsson with her breakfast set up. Enter her room, greet her, and let her know that it’s time for breakfast. Respond to the situation you are presented with.
ROLE PLAY 6: CLIENT ROLE CARD
Your name is Erika Karlsson. After the HCA lets you know that it’s time for breakfast, tell her you don’t feel hungry. When the HCA follows up, tell her that you have a stomach ache.
CLIENT PROFILES
ROLE PLAY 1: CLIENT PROFILE
Jenny Smith is a 76-year-old female who lives alone.
Health challenges/diagnosis: Diabetes, neuropathy, significant visual impairment, history of falls, history of depression
ADLs: Partial assist with personal care
Mobility: One person assist with walker, unsteady on feet, history of falls
Nutrition: Diabetic diet, receives Meals on Wheels, family sometimes brings food (sweets), Jenny occasionally skips meals
Communication: English
ROLE PLAY 2: CLIENT PROFILE
Ali Singh is a 92-year-old female living in an assisted living residence.
Health challenges/diagnosis: Parkinson’s disease with history of falls, arteriosclerotic heart disease, orthostatic hypotension
ADLs: Supervision in bathroom, requires cueing, appropriate cultural attire, raised toilet seat, meal set up
Mobility: Uses four-wheeled walker
Nutrition: Soft diet with fluids, plate protector, adaptive utensils, cup with lid
Communication: Speaks Punjabi and English
Cultural: Attends temple every Sunday
ROLE PLAY 3: CLIENT PROFILE
Aiko Tanaka is a 42-year-old female client who lives in a group home.
Health challenges/diagnosis: Ataxic cerebral palsy, expressive aphasia
ADLs: Full assist with personal care
Mobility: Risk of falls, assist with range of motion exercises
Nutrition: Soft diet, encourage small snacks throughout the day
Communication: Understands English and Japanese, uses gestures to communicate when hungry
ROLE PLAY 4: CLIENT PROFILE
Matika Tahoma is a 73-year-old male in hospital following hip replacement surgery.
Health challenges/diagnosis: Osteoarthritis, history of falls, CVA at age 68, dysphagia
ADLs: Assist client to sit (dangle) at side of bed (Q.I.D), one-person assist for dressing, assist with mouth care, commode for toileting, and deep breathing and coughing exercises
Mobility: Two-person assist to dangle and commode
Nutrition: Thickened fluids, dysphagia diet
Communication: Speaks Halkomelem and English
ROLE PLAY 5: CLIENT PROFILE
Gabriela Martinez is a 79-year-old female who lives in an complex care residence.
Health challenges/diagnosis: Blind due to glaucoma, history of urinary tract infections
ADLs: Requires partial assistance with personal hygiene
Mobility: Uses white cane, assist with walking
Nutrition: Assist with meal set up/eating, record fluid intake, cranberry juice with meals
Communication: Speaks Spanish and English
ROLE PLAY 6: CLIENT PROFILE
Erika Karlsson is an 88-year-old female who lives in residential care.
Health challenges/diagnosis: Arthritis, esophageal reflux, constipation, hemorrhoids
ADLs: Partial bath, set up with meals, assist with hearing aid and glasses
Mobility: Uses four-wheeled walker, assist with mobility
Nutrition: Low-fibre diet, small appetite, encourage to drink fluids
Communication:Speaks Swedish and English, but is quiet and doesn’t like to bother staff
Other: Last recorded bowel movement was four days ago
5. Case Study: Decision-Making Regarding Reporting Changing Client Condition
The following case study is used with permission of Island Health.
It is not unusual for client status to change quickly in acute care settings; HCAs need to know to most effectively communicate changes in client conditions to ensure their safety and well-being.
For the past few months, Mel, an HCA, has been working full time on a surgical unit. They are getting to know the team members and enjoy the opportunity to work in partnership with the health care team.
For the past few shifts, Mel has been supporting Mr. Hassan. Mr. Hassan is 67 years old and is a retired teacher. He had surgery six days ago to remove a tumour in his small intestine and now has a colostomy bag. He has been progressing well after the surgery and is looking forward to returning home to his wife. Mr. Hassan plans to independently manage his colostomy care with assistance from community-based nursing as required.
Mel is stopped by Mr. Hassan while doing their hourly care rounds. Mr. Hassan indicates that he is feeling like he is going to vomit and needs help. Mr. Hassan’s RN, Indira, is currently in a family meeting with another patient.
Ask students to consider the “who, what, when, where, why and how” for this situation.
Who to communicate with. It is important to get the assistance of nursing staff with this as there may be a variety of factors contributing to the nausea. If they are unable to interrupt Indira, they should contact the RN who is covering for Indira or the team leader.
What to communicate. Tell the RN what you saw (observations), when you saw it, and what Mr. Hassan reported to you regarding his nausea. Determine if the RN wants you to record this on any special forms. Be prepared to answer some questions from the RN.
When. This nausea is a change for Mr. Hassan. Because of this, it is important that you verbally communicate this information immediately.
Where. You may be asked to record this information on a special form or chart. Depending on the outcome, this may be a topic that is addressed in a team huddle. Collaborate with the RN to determine who will report this information and where. Ensure patient confidentiality and privacy is respected during verbal communication.
Why. It is critical that this information is shared in a timely way as Mr. Hassan will require the assessment of his condition and possible treatment. Timely communication will also reassure Mr. Hassan that his care needs are being addressed.
How. You may be able to use the nurse call bell system, a pager, or a voice-activated device to alert team members that you require assistance.
Consider what forms and meetings you can use to share information once immediate needs are addressed.
Strategies that Focus on Professional Approaches to Practice
1. The Dance: Maintaining Professional Boundaries
Maintaining professional boundaries when caring for a dying person can sometimes be particularly challenging. Elizabeth Causton, in her writings on the “The Dance” (See STUDENT HANDOUT 2), provides caregivers with a metaphor that may be helpful as they work closely with clients and families.
Have students read the description of “The Dance” and ask them to discuss the following:
- Does the metaphor of the dance make sense in relation to professional practice when caring for dying individuals?
- What does the author mean by “hooks” in this context? Can you think of any hooks that might affect you in an end-of-life context?
- Have you seen or could you envision caregiver behaviours, such as those described, that reflect a lack of perspective? How would a caregiver behave who is kind, compassionate, and caring yet maintains professional boundaries – who is able to “feel deeply and to act wisely”?
- How might the ideas in this reading apply to other caregiving contexts (e.g., with clients who are vulnerable but not necessarily dying)?
STUDENT HANDOUT 2
The Dance by Elizabeth Causton
When we work with a conscious awareness of where we stand in relationship to patients and families, respecting their unique “dance” in response to grief and loss, we are less likely to become over involved or to get lost in our work.
The idea of a family dance is not new, but it works particularly well as an image that reminds us of the importance of paying attention to boundaries as we work with people who are “vulnerable and broken.” The image can also be used to describe the sense of continuity of the family dance, which has evolved over generations. It reminds us that every family dance has its own history and that every step taken on the family dance floor has a reason in the context of that shared history.
So, when one member of the family either sits down or lies down on the dance floor because of terminal illness, the dance may look quite clumsy as the family tries to modify their routine to accommodate the changes, but the new steps are not random. They, too, have meaning in the context of what has gone on before.
Still, as we watch families struggle with a difficult dance to music that always gets faster and louder in a crisis, we may be tempted to get onto their dance floor to try and teach them a new dance, with steps from the dance that we are most familiar with – our own. Of course, this rarely works, for the obvious reason that our dance steps do not have a history or a reason in the context of another family’s particular dance. Our valuable and unique perspective is lost the moment we step out onto someone else’s dance floor. Regardless of our good intentions, we truly become lost in our work.
The greater value of our role is to stay on the edge of the dance floor and from that vantage point, to observe, comment on, and normalize the process that the family is going through. We may suggest options, new dance steps that the family hasn’t thought of, but we do so with the recognition that they can only consider new ideas in the context of their own history. This is what it means to work from a “therapeutic distance,” to work with an awareness of where we stand in relation to the people with whom we are working.
However, whereas working with this kind of clarity and respect for boundaries may be our goal, experience tells us that it is not easy to achieve. The edge of the family dance floor is often, in fact, a fluid border as difficult to define as it is to say exactly where the sea meets the sand. In addition, each of us has “hooks” – people or situations that may touch us in some deep, unconscious place. Because we have an obligation to do this work with awareness, it is important that we do our “homework,” seeking to identify our “hooks” and paying attention to signs that we may have stepped over the line.
The signs that we are losing our perspective are: 1) experiencing an extreme emotional reaction to a person or situation that (perhaps without our knowing it) resonates with an unresolved issue or a difficult relationship on our own dance floor; 2) feeling a sense of ownership as reflected in language such as “my patients” or “my families,” or difficulty in letting go or sharing individuals with other team members; and/or 3) experiencing a need to influence or control patients and families by directing their options and choices or by making ourselves indispensable to them.
Despite having identified signs of over-involvement, it is also important to understand the challenges inherent in our work and be gentle with ourselves as we strive to be “good enough.” We need to remember that maintaining a therapeutic distance does not preclude strong emotions and deep caring. Two of the great advantages of knowing where we stand and being clear about what we bring to our work are being able both to feel deeply and to act wisely.
Reprinted with permission of the author
Elizabeth Causton
elizabeth@caustonsonbeach.ca
Causton, Elizabeth. (2003). The Dance. In M. Cairns; M. Thompson; W. Wainwright (Eds.), Transitions in Dying and Bereavement: A Psychosocial Guide for Hospice and Palliative Care. (p. 202–203) Baltimore, MD: Health Professions Press.
Suggested Course Assessments
The course learning outcomes may be assessed by the following tasks:
- One or more quizzes or examinations that pertain to knowledge of human anatomy and physiology, normal changes of aging, special diets, diversity and dietary needs, common challenges to health and healing, and palliative care (Learning Outcomes 1, 2, 3, and 4).
- An assignment in which students, working in small groups, research a common health challenge and present their findings to the class. Each group should consider dietary needs as they relate to specific health challenges and how the health challenge could impact the physical, psychological, cognitive, social, spiritual dimensions of the individual’s health. Each group should also identify community resources and discuss the HCA role in caring for and supporting individuals experiencing the health challenge (Learning Outcomes 2, 3, and 4).
- A written assignment in which each student identifies what they would want in a care provider for themselves or a close family member who is dying. Each student will discuss this fictitious “perfect” caregiver in terms of the person’s:
- Comfort with the death and the dying process
- Knowledge of and ability to provide palliative care
- Ability to communicate with the dying individual
- Relationship with other health team members
- Relationship with family members
- Ability to communicate with family members during the dying process and immediately after the death of the client
- Ability to adapt to cultural, religious, or other person-centred care requirements
Each student should reflect on their strengths as a caregiver as these relate to end-of-life care and identify areas of personal or professional development that would assist them to become more effective or confident in providing end-of-life care (Learning Outcome 4).
Resources for Common Health Challenges
Online Resources
ALS Canada. https://www.als.ca/
American Psychological Association. (2019). Culturally diverse communities and palliative and end-of-life care [Fact sheet]. https://www.apa.org/pi/aging/programs/eol/end-of-life-diversity.pdf
Arthritis Canada. https://arthritis.ca/
Association of Canadian Community Colleges and Canadian Association of Continuing Care Educators. (2012, June 28). Canadian educational standards for personal care providers. https://www.collegesinstitutes.ca/wp-content/uploads/2014/05/Reference-Guide_Canadian-Educational-Standards-for-Personal-Care-Providers_ACCC.pdf
BC Centre for Disease Control. (2024.). Communicable diseases: Reportable communicable diseases in BC. http://www.bccdc.ca/health-professionals/data-reports/communicable-diseases
British Columbia Hospice Palliative Care Association. https://bchpca.org/
Canadian Cancer Society. https://www.cancer.ca/
Canadian Hospice Palliative Care Association. https://www.chpca.ca/
Canadian Liver Foundation. https://www.liver.ca/
Canadian Lung Association. https://www.lung.ca/
CDC: Centers for Disease Control and Prevention. (2023). Understanding blood clots. https://www.cdc.gov/blood-clots/toolkit/understanding-blood-clots-infographic.html?CDC_AAref_Val=https://www.cdc.gov/ncbddd/dvt/understanding-blood-clots-infographic.html
Challacombe, L. (2021). The epidemiology of HIV in Canada [Fact sheet]. CATIE. https://www.catie.ca/en/fact-sheets/epidemiology/epidemiology-hiv-canada
Christianson, T. & Morris, K. (2023). Personal care skills for health care assistants: 6.4 special diets. https://hcalabtheoryandpractice.pressbooks.tru.ca/chapter/special-diets/
Cleveland Clinic. (2023). Diarrhea. https://my.clevelandclinic.org/health/diseases/4108-diarrhea
Cleveland Clinic. (2022). Edema. https://my.clevelandclinic.org/health/diseases/12564-edema
College & Institutes Canada (CICAN). (2022). National occupational standard for personal care providers. https://nos-nnp.ca/standard/
Diabetes Canada. https://www.diabetes.ca/
Diabetes Canada. (2021). Basic meal planning [Blog post]. http://www.diabetes.ca/diabetes-and-you/healthy-living-resources/diet-nutrition/basic-meal-planning
Dodd, K. (2020). End of life nutrition [Blog post]. The Geriatric Dietitian. https://www.thegeriatricdietitian.com/embracing-hospice-end-of-life-nutrition/
Dying with Dignity Canada. https://www.dyingwithdignity.ca/
Emedicinehealth. (2017). HIV and AIDS quiz: HIV testing and symptoms [Online quiz]. http://www.emedicinehealth.com/hiv-aids_quiz_iq/quiz.htm
FHNA. (n.d.) Preparing for the Journey: Wholistic end-of-life care for First National people living in BC. https://www.fnha.ca/Documents/FNHA-Preparing-for-the-Journey-Booklet.pdf
Government of British Columbia. (2022, July 19). Advance care planning. https://www2.gov.bc.ca/gov/content/family-social-supports/seniors/health-safety/advance-care-planning
Government of British Columbia. (n.d.). Cultures, food traditions and healthy eating. https://food-guide.canada.ca/en/healthy-eating-recommendations/enjoy-your-food/cultures-food-traditions-and-healthy-eating/
Government of British Columbia. (2023, December 18). Medical assistance in dying. https://www2.gov.bc.ca/gov/content/health/accessing-health-care/home-community-care/care-options-and-cost/end-of-life-care/medical-assistance-in-dying
Government of Canada. (2023). End of life care. https://www.canada.ca/en/health-canada/topics/end-life-care.html
HealthLinkBC. https://www.healthlinkbc.ca/
HealthLinkBC. (n.d.). Seniors’ health. https://www.healthlinkbc.ca/health-topics/common-health-concerns/seniors
Heart and Stroke Foundation. https://www.heartandstroke.ca/
Interior Health Authority. (2021). Palliative and end of life care to relieve suffering and improve quality of life. https://www.interiorhealth.ca/YourCare/PalliativeCare/Pages/default.aspx
Johns Hopkins Medicine. (2024). Constipation. https://www.hopkinsmedicine.org/health/conditions-and-diseases/constipation
Kidney Foundation of Canada. https://kidney.ca/
Mayo Clinic. (2017). Diseases and conditions [Index]. https://www.mayoclinic.org/diseases-conditions/index?letter=A
Medical News Today. (2017). What causes difficulty swallowing (dysphagia)? http://www.medicalnewstoday.com/articles/177473.php
MS Society. https://mssociety.ca/
Muscular Dystrophy Association. https://www.mda.org/
NIH: National Institute of Diabetes and Digestive and Kidney Disease. (n.d.). Health Information. https://www.niddk.nih.gov/health-information
Osteoporosis Canada. https://osteoporosis.ca/
PAN (Pacific AIDS Network). https://pacificaidsnetwork.org/
Pain B.C. https://www.painbc.ca/
Parkinson Society British Columbia. https://www.parkinson.bc.ca/
Provincial Health Services Authority. (2024). Medical assistance in dying. http://www.phsa.ca/health-info/medical-assistance-in-dying
Public Health Agency of Canada. (2023). Healthcare infection prevention and control guidelines. https://www.canada.ca/en/public-health/services/infectious-diseases/nosocomial-occupational-infections.html
Public Health Agency of Canada. (2022). Infectious diseases. https://www.canada.ca/en/public-health/services/infectious-diseases.html
Public Health Association of BC. (2024). ImmunizeBC. https://immunizebc.ca/
Quizlet Inc. [Mobile app]. https://quizlet.com/
St. George’s University. (2021). 75 must-know medical terms, abbreviations, and acronyms. https://www.sgu.edu/blog/medical/medical-terms-abbreviations-and-acronyms/
UpToDate. (2024). Patient education: Edema (Swelling) (Beyond the basics) https://www.uptodate.com/contents/edema-swelling-beyond-the-basics/print
Victoria Hospice. https://victoriahospice.org/
Warick, J. (2023, June 4). A good death. CBC News. https://www.cbc.ca/newsinteractives/features/a-good-death-maid
Online Videos
CrashCourse. (2021). How do outbreaks start? Pathogens and immunology: Crash Course outbreak science #2 [Video]. YouTube. https://www.youtube.com/watch?v=40cyYqqQmJ4
CrashCourse. (2021). What is outbreak science: Crash Course outbreak science #1. [Video]. YouTube. https://www.youtube.com/watch?v=_qAzXb7mA2g
Diseases Simplified. (2020, January 16). Must know causes of edema/swelling [Video]. YouTube. https://www.youtube.com/watch?v=jyoaxSbwFTM
Dr. Pauline Moyaert. (2022). What are the last days before death like? Signs of approaching death [Video]. YouTube. https://www.youtube.com/watch?v=JDirQOmydRs
DW Documentary. (2024). Meeting death on our own terms [Video]. YouTube. https://www.youtube.com/watch?v=2uI5k-mfHBI
End of Life Project. (2012, November 29). Completing the circle: End of life care with Aboriginal families [Video]. YouTube. https://www.youtube.com/watch?v=XbUGMIKId0c
Geriatric Dietitian. (2019, July 20). Embracing hospice end of life nutrition [Video]. YouTube. https://www.youtube.com/watch?v=suj_EXYHhGI
Gilbert, D. (2014, February 18). Loss of independence within the elderly [Video]. YouTube. https://www.youtube.com/watch?v=up7rGG0ytoE
Halton Healthcare. (2020, February 20). Pressure injury prevention 2020 [Video]. YouTube. https://www.youtube.com/watch?v=qcyhJuNhPG4
Heat Inc., Health Education and Training. (2017, September 11). The nursing assistant: Pressure ulcer prevention [Video]. YouTube. https://www.youtube.com/watch?v=6OGSkxlr9-c
HeistheStud. (2014, December 14). Emphysema & bronchitis [Video]. YouTube. https://www.youtube.com/watch?v=S-tryBgTBBk
Human Biology Explained. (2014, March 8). Anatomical terms – drawn and defined (updated). [Video]. YouTube. https://www.youtube.com/watch?v=kvHWnJwBkmo&app=desktop
Huntington’s Disease. (2021). Heather’s story: Family matters – Huntington’s Disease awareness month 2021. [Video]. YouTube. https://www.youtube.com/watch?v=TwNyNsKGxeo
Innovative Hearing Solutions, Inc. (2015, July 14). Inserting and removing RIC’s, CIC’s and BTE’s hearing aids [Video]. YouTube. https://www.youtube.com/watch?v=K4BK-ohwhoI
Interior Health. (2016). Advance care planning (ACP) and MOST – Info for patients. [Video]. YouTube. https://www.youtube.com/watch?v=Y0TyhWQOf_8
Janux. (2015, January 10). Human physiology – Introduction to the immune system. [Video]. YouTube. https://youtu.be/CG931UYMbN0
The Lancet. (2022). A new version of death and dying. [Video]. YouTube. https://www.youtube.com/watch?v=dRqjkIPMBhw
Life Before Death. (2013, December 7). Life before death – Roger’s story [Video]. YouTube. https://www.youtube.com/watch?v=eQRHrgCiEzI
LivingHealthyChicago. (2016, March 7). Living with arthritis [Video]. YouTube. https://www.youtube.com/watch?v=D6HtMELddcg
Miller, B. (2015, March). What really matters at the end of life [Video]. TED2015. https://www.ted.com/talks/bj_miller_what_really_matters_at_the_end_of_life
MooMooMath and Science. (2017, May 18). Types of human body tissues [Video]. YouTube. https://www.youtube.com/watch?v=O0ZvbPak4ck
NBC News. (2019). How an ALS patient battled with choosing his last day. [Video]. YouTube. https://www.youtube.com/watch?v=VKDDgXRRfeM&t=130s
Northwestern Medical. (2020). Visualizing visual impairment [Video]. YouTube. https://www.youtube.com/watch?v=OkeqHe53I1w
Northwestern Medical. (2021). Visualizing visual impairments: Part 2 [Video]. YouTube. https://www.youtube.com/watch?v=xk-Ix1wv1O8
Northern Health BC. (2016). Cultural practices around illness and death [Video]. YouTube. https://www.youtube.com/watch?v=gdjnSp3Wxd8
Nutrition Facts. (2024). How to die a good death [Video]. YouTube. https://www.youtube.com/watch?v=S57HxdaOPHM
NPT Reports. (2013, September 13). End of life. Aging matters NPT reports. [Video]. YouTube. https://www.youtube.com/watch?v=uzfcvptgJ2c
PBS Digital Studios. (2013, March 25). You are mainly microbe! [Video]. YouTube. https://youtu.be/4BZME8H7-KU
Palliative Care Australia. (2018). Myth: Pain is an inevitable part of dying [Video]. YouTube. https://www.youtube.com/watch?v=Iuu3YGayqYc
Schwenke, T. (2024). Human nervous system (Part 1). Spinal cord and periphery animation. [Video]. YouTube. https://www.youtube.com/watch?v=_Dhj-RqfGe4
Schwenke, T. (2024). Human nervous system (Part 2). Brain animation [Video]. YouTube. https://www.youtube.com/watch?v=CurW-sIQPxU
The Jackson Laboratory. (2022). What is cancer? [Video]. YouTube. https://www.youtube.com/watch?v=BttAtBZeQc4
St. John’s Hospice. (2020). Nutrition and fluids at end of life – Care home support [Video]. YouTube. https://www.youtube.com/watch?v=kLEpXk1mRRo&t=55s
St. Michael’s Hospital. (2018, August 2). What is hypoglycemia? – DiaBiteSize [Video]. YouTube. https://www.youtube.com/watch?v=e0XN_hjfQiA&feature=youtu.be
Sunnybrook Hospital. (2018, March 13). Quality dying – Let’s talk about it [Video]. YouTube. https://www.youtube.com/watch?v=9CYl12mBluA
TED-Ed. (2014, November 10). How a wound heals itself – Sarthak Sinha [Video]. YouTube. https://www.youtube.com/watch?v=TLVwELDMDWs
TED-Ed. (2014, November 24). How do lungs work? – Emma Bryce [Video]. YouTube. https://youtu.be/8NUxvJS-_0k
TED-Ed. (2017, December 14). How your digestive system works – Emma Bryce [Video]. YouTube. https://www.youtube.com/watch?v=Og5xAdC8EUI
TED-Ed. (2018, March 12). The science of skin – Emma Bryce [Video]. YouTube. https://youtu.be/ OxPlCkTKhzY
Teepa Snow’s Positive Approach to Care. (2017, December 21). How dementia affects language skills [Video]. YouTube. https://www.youtube.com/watch?v=0BlZF_4EKp4
USMLE pass. (2019, November 18). Sounds of breathing patterns (Cheyne-Stokes, Kussmauls, Biots) [Video]. YouTube. https://www.youtube.com/watch?v=ViGjOiPE2mY
Whitford, B. and Paskievich, J. (Directors). (2005). The gift of diabetes [Film]. National Film Board. https://www.nf b.ca/film/gift_of_diabetes/
YourRenalCare. (2011, December 15). Kidney stones [Video]. YouTube. https://www.youtube.com/watch?v=LngI brHJkXoE
Online Learning Tools
The following materials are either ready for use in the classroom or represent a large repository of resources on multiple topics. A brief description and estimated time for each resource is included for each.
Canadian Virtual Hospice. (2024).
This website provides several valuable resources regarding palliative care, including the four resources below.
- Living my culture.
- A series of online videos discussing quality palliative care for people from the following cultures: First Nations, Inuit, Métis, Chinese, Ethiopian, Filipino, Indian, Iranian, Italian, Pakistani, Somali. videos range from 2 to 25 minutes.
- Grief in 2SLGBTQ+ communities.
- This module includes eight chapters exploring grief in 2SLGBTQ+ communities. Stories, guidelines, and videos are provided.
- My grief.
- This section includes 28 modules covering topics from the basics of grief, to personal grief, grief caused by specific circumstances and MAID. Modules include a combination of stories, guidelines, and videos.
- The Learning Hub: Indigenous cultural safety training.
- This section provides modules on grief and palliative practices specific to Indigenous persons. (Note: This Learning Hub is not the same as the Provincial Health Services Authority LearningHub website.)
CrashCourse. (2015). Anatomy & physiology.
- An educational website including a series of 47 animated videos covering the types of tissues, organs and systems in the human body. They range from 2 to 12 minutes in length.
Demystifying Medicine McMaster. (n.d.).
A YouTube channel with hundreds of videos on health and medical content created by undergraduate and graduate students at McMaster University. Topics include anatomy, genetic disorders, physical, cognitive, and mental health conditions and diseases, and nutrition and health.
LearningHub, Provincial Health Services Authority
LearningHub is a secure, province-wide course registry and learning management system hosted by the Provincial Health Services Authority. LearningHub provides a wide range of online and in-class courses on various topics. These e-learning courses can be used as activities or assessments for the HCA program courses. Students can access the LearningHub using their post-secondary email account. After completing all mandatory learning activities for a course, students can obtain a course completion certificate to show that they fulfilled all the course requirements. Instructions for registering and completing courses are available on the LearningHub site.
- Fraser Health biological hazards and communicable disease. (45 minutes)
- Introduction to palliative care. (45 minutes).
- Introduction to medical assistance in dying: MAiD. (15 minutes).
- NHA-CL-Palliative care awareness. (90 minutes)
Medical Centric. (n.d.). Awesome medical content.
- A YouTube channel with hundreds of videos on health and medical content. Topics include anatomy, pathophysiology, nutritional concerns, and oral health. The content is created by medical professionals and designed for the patients and the public.
- A YouTube channel hosting 30 videos by the Pallium Foundation of Canada exploring palliative care. Although these videos are older (12-16 years old), six of the videos specifically focus on palliative care and Indigenous persons. Although the visual effects are fuzzy, the content is valuable.
Science ABC. (2024). Human body. [Video series].
- A series of 13 videos between 5 to 9 minutes on the systems in the human body.
Stories for Caregivers. (2024).
- This website has a collection of videos about patients and caregivers, covering a wide range of health challenges.
