Chapter 6. States of Consciousness
Sleep and Why We Need Sleep
Jessica Motherwell McFarlane
Approximate reading time: 47 minutes
We spend approximately one-third of our lives sleeping. Given that the average life expectancy for Canadian citizens is about 82 years of age (Statistics Canada, 2018), we can expect to spend approximately 25+ years of our lives sleeping. Some animals never sleep (e.g., some fish and amphibian species); other animals sleep very little without apparent negative consequences (e.g., giraffes). Why do we devote so much time to sleeping? Is it absolutely essential that we sleep? This section will consider these questions and explore various explanations for why we sleep.
What is Sleep?
You have read that sleep is distinguished by low levels of physical activity and reduced sensory awareness. As discussed by Siegel (2008), a definition of sleep must also include mention of the back and forth actions of the circadian (daily cycles) and homeostatic (balancing) mechanisms that regulate sleep. Homeostatic regulation of sleep is evidenced by sleep rebound following sleep deprivation. Sleep rebound refers to the fact that a sleep-deprived individual will fall asleep more quickly during subsequent opportunities for sleep. Sleep is characterised by certain patterns of activity of the brain that can be visualized using electroencephalography (EEG), and different phases of sleep can be differentiated using EEG as well.
Sleep-wake cycles seem to be controlled by multiple brain areas acting in conjunction with one another. Some of these areas include the thalamus, the hypothalamus, and the pons. As mentioned previously, the hypothalamus contains the SCN — the biological clock of the body — in addition to other nuclei that, in conjunction with the thalamus, regulate slow-wave sleep. The pons is important for regulating rapid eye movement (REM) sleep (National Institutes of Health, n.d.).
Sleep is also associated with the secretion and regulation of a number of hormones from several endocrine glands including: melatonin, follicle stimulating hormone (FSH), luteinising hormone (LH), and growth hormone (National Institutes of Health, n.d.). You have read that the pineal gland releases melatonin during sleep (Figure SC.9). Melatonin is thought to be involved in the regulation of various biological rhythms and the immune system (Hardeland et al., 2006). During sleep, the pituitary gland also secretes both FSH and LH, which are important in regulating the reproductive system (Christensen et al., 2012; Sofikitis et al., 2008). The pituitary gland also secretes growth hormone during sleep, which plays a role in physical growth and maturation as well as other metabolic processes (Bartke, Sun, & Longo, 2013).
An illustration of a brain shows the locations of the hypothalamus, thalamus, pons, suprachiasmatic nucleus, pituitary gland, and pineal gland.
, pituitary gland, and pons labelled.")
Why Do We Sleep?
Given the central role that sleep plays in our lives and the number of adverse consequences that have been associated with sleep deprivation, one would think that we would have a clear understanding of why it is that we sleep. Unfortunately, this is not the case.
Cognitive Function of Sleep
One theory regarding why we sleep involves sleep’s importance for cognitive function and memory formation (Rattenborg, Lesku, Martinez-Gonzalez, & Lima, 2007; Schreiner, Lehmann, & Rasch, 2017). We know that sleep deprivation disrupts cognition and creates memory deficits (Brown, 2012), leading to impairments in our abilities to maintain attention, make decisions, and recall long-term memories. These impairments become more severe as the amount of sleep deprivation increases (Alhola & Polo-Kantola, 2007). Furthermore, slow-wave sleep after learning a new task can improve resultant performance on that task (Huber, Ghilardi, Massimini, & Tononi, 2004) and seems essential for effective memory formation (Stickgold, 2005). Given this strong association between sleep and cognitive performance we could theorise that one purpose of sleep is to promote memory and optimal cognitive performance. Perhaps cramming all night for a test may not be effective, and could even prove counterproductive.
It is possible that sleep serves no single universally adaptive function; there are many benefits associated with adequate amounts of sleep. Different species have evolved different patterns of sleep in response to their unique evolutionary pressures.
Getting the optimal amount of sleep has also been associated with other cognitive benefits. Research indicates that these possible benefits include: increased capacities for creative thinking (Cai, Mednick, Harrison, Kanady, & Mednick, 2009; Wagner, Gais, Haider, Verleger, & Born, 2004);, language learning (Fenn, Nusbaum, & Margoliash, 2003; Gómez, Bootzin, & Nadel, 2006; Kurdziel, Mantua, & Spencer, 2017); and inferential judgments (Ellenbogen, Hu, Payne, Titone, & Walker, 2007). Interestingly, one study found that a 90-minute nap after vocabulary learning significantly improved performance compared to rest or interference (Heim et al., 2017). It is possible that even the processing of emotional information is influenced by certain aspects of sleep (Walker, 2009).
Do you notice benefits in your ability to study if you take a 90-minute nap?
Watch this video: To Sleep, Perchance to Dream: Crash Course Psychology #9 (10.5 minutes)
“To Sleep, Perchance to Dream: Crash Course Psychology #9” video by CrashCourse is licensed under the Standard YouTube licence.
Stages of Sleep
Glossary of Sleep Terms
- Alpha Waves: These are brain waves that are present when a person is relaxed and awake, but not actively processing information. They are typically seen when someone is calm, meditative, or just beginning to drift off to sleep.
- Delta Waves: These are the slowest and highest amplitude brain waves, characteristic of deep, restorative sleep. They dominate during the deepest stages of non-REM sleep, and are crucial for feeling refreshed and restored upon waking.
- Theta Waves: These brain waves are associated with the early stages of sleep, particularly stages 1 and 2 of non-REM sleep. They represent a state of light sleep or drowsiness, where a person can be easily awakened.
- K-complexes: These are singular, high amplitude waves that occur during stage 2 of non-REM sleep. K-complexes are thought to represent a mechanism for maintaining sleep in the presence of external stimuli and aiding in sleep-based memory consolidation.
- Sleep Spindles: These are bursts of rapid, rhythmic brain activity that occur during stage 2 of non-REM sleep. Sleep spindles are believed to play a role in integrating and processing memories and information learned throughout the day.
- Non-REM Sleep: This phase encompasses the first four stages of the sleep cycle. It begins with light sleep (stages 1 and 2), marked by theta waves, and progresses into deep sleep, characterised by delta waves. Non-REM sleep is crucial for physical restoration and memory consolidation.
- REM Sleep (Rapid Eye Movement Sleep): This is a unique phase of sleep characterised by rapid movements of the eyes, low muscle tone, and the propensity to dream vividly. It occurs cyclically throughout the night, with longer periods towards the morning. REM sleep is essential for cognitive functions like memory, learning, and creativity.
Sleep is not a uniform state of being. Instead, sleep is composed of several different stages that can be differentiated from one another by the patterns of brain wave activity that occur during each stage. These changes in brain wave activity can be visualised using Electroencephalography (EEG — see text box for definition) and are distinguished from one another by both the frequency and amplitude of brain waves (Figure SC.8).
What are Waves and Hertz (Hz)?
First, think of waves as patterns of energy moving through space or along a medium, like the ripples on a pond after you throw a stone into it. These waves can be measured in several ways, but two key aspects are their frequency and amplitude.
Frequency refers to how many waves pass a certain point in a specific amount of time. Imagine standing by the pond and counting how many ripples pass by you in one second. In the context of brain waves, we measure frequency in hertz (Hz), which is the unit of measurement for frequency. One hertz equals one wave cycle per second. So, when we say brain waves are 8 Hz, it means eight cycles of that wave pattern occur in one second.
Amplitude is about the height of the waves. In our pond analogy, it’s how big the ripples are. For brain waves, a higher amplitude means a stronger or more pronounced wave.
Tools for Measuring Brain Waves
Scientists use a tool called an EEG (electroencephalogram) to measure brain waves. This device (which looks like a cap with many wires attached) can detect the electrical activity in your brain by using small sensors attached to the scalp. The EEG records the brain’s activity and shows it as wavy lines on a monitor or paper. By looking at these lines, scientists can measure the frequency and amplitude of your brain waves.
Why It Matters
Understanding the frequency and amplitude of brain waves helps scientists and doctors learn about different states of consciousness, like being awake, relaxed, or in various stages of sleep. It also helps in diagnosing and treating certain brain-related conditions. By measuring these waves, we gain insights into how the brain works, how we think, feel, and process the world around us. It’s a crucial part of neuroscience that helps unravel the mysteries of the human brain.
Sleep can be divided into two different general phases: REM sleep and non-REM (NREM) sleep. Rapid eye movement (REM) sleep is characterised by darting movements of the eyes under closed eyelids. Brain waves during REM sleep appear very similar to brain waves during wakefulness. In contrast, non-REM (NREM) sleep is subdivided into three stages distinguished from each other and from wakefulness by characteristic patterns of brain waves. The first three stages of sleep are NREM sleep, while the fourth and final stage of sleep is REM sleep. In this section, we will discuss each of these stages of sleep and their associated patterns of brain wave activity.
NREM Sleep
Stage N1 – Transition to sleep
The first stage of NREM sleep is known as stage 1 sleep. Stage 1 sleep is a transitional phase that occurs between wakefulness and sleep, the period during which we drift off to sleep. During this time, there is a slowdown in both the rates of respiration and heartbeat. In addition, stage 1 sleep involves a marked decrease in both overall muscle tension and core body temperature.
In terms of brain wave activity, stage 1 sleep is associated with both alpha and theta waves. The early portion of stage 1 sleep produces alpha waves, which are relatively low frequency (8–13 Hz), high amplitude patterns of electrical activity (waves) that become synchronized (Figure SC.11). This pattern of brain wave activity resembles that of someone who is very relaxed, yet awake. As an individual continues through stage 1 sleep, there is an increase in theta wave activity. Theta waves are even lower frequency (4–7 Hz), higher amplitude brain waves than alpha waves. It is relatively easy to wake someone from stage 1 sleep; in fact, people often report that they have not been asleep if they are awoken during stage 1 sleep.
 Plotted along the y-axis and moving upward are the stages of sleep. First is REM, followed by Stage 3 NREM Delta, Stage 2 NREM Theta (sleep spindles; K-complexes), Stage 1 NREM Alpha, and Awake. Charted on the x axis is Time in seconds from 2–20 in 2 second intervals. Each sleep stage has associated wavelengths of varying amplitude and frequency. Relative to the others, “awake” has a very close wavelength and a medium amplitude. Stage 1 is characterised by a generally uniform wavelength and a relatively low amplitude, which doubles and quickly reverts to normal every 2 seconds. Stage 2 consists of a similar wavelength as stage 1. It introduces the K-complex from seconds 10 through 12, which is a short burst of doubled or tripled amplitude and decreased wavelength. Stage 3 has a more uniform wave with gradually increasing amplitude. Finally, REM sleep looks much like stage 2 without the K-complex.")
Stage N2 – Light Sleep
As we move into stage 2 sleep, the body goes into a state of deep relaxation. Theta waves still dominate the activity of the brain, but they are interrupted by brief bursts of activity known as sleep spindles (Figure SC.12). A sleep spindle is a rapid burst of higher frequency brain waves that may be important for learning and memory (Fogel & Smith, 2011; Poe, Walsh, & Bjorness, 2010). In addition, the appearance of K-complexes is often associated with stage 2 sleep. A K-complex is a very high amplitude pattern of brain activity that may in some cases occur in response to environmental stimuli. Thus, K-complexes might serve as a bridge to higher levels of arousal in response to what is going on in our environments (Halász, 1993; Steriade & Amzica, 1998).

Stage N3 – Deep sleep (formerly Stage 3+4)
Non-REM sleep is often referred to as deep sleep or slow-wave sleep because this stage is characterised by low frequency (less than 3 Hz), high amplitude delta waves (Figure SC.13). During this time, an individual’s heart rate and respiration slow dramatically. It is much more difficult to wake someone from deep sleep during non-REM than during earlier stages. Interestingly, individuals who have increased levels of alpha brain wave activity (more often associated with wakefulness and transition into stage 1 sleep) during non-REM often report that they do not feel refreshed upon waking, regardless of how long they slept (Stone, Taylor, McCrae, Kalsekar, & Lichstein, 2008). It is worth noting that sometimes you may see slow-wave sleep divided into two stages, rather than just one. Previously, researchers distinguished between stages 3 and 4 as being characterised by increased delta waves. However, it is now accepted as a single stage, non-REM, known as slow-wave sleep.
 shows the pattern of delta waves, which are low frequency and high amplitude. Delta waves are found mostly in non-REM of sleep. Chart (b) shows brainwaves at various stages of sleep, with non-REM highlighted.")
REM Sleep
As mentioned earlier, REM sleep is marked by rapid movements of the eyes. The brain waves associated with this stage of sleep are very similar to those observed when a person is awake, as shown in Figure SC.14; this is the period of sleep in which dreaming occurs. It is also associated with paralysis of muscle systems in the body, with the exception of those that make circulation and respiration possible. Therefore, no voluntary movement of muscles occurs during REM sleep in a normal individual; REM sleep is often referred to as paradoxical sleep because of this combination of high brain activity and lack of muscle tone. Like NREM sleep, REM has been implicated in various aspects of learning and memory (Wagner, Gais, & Born, 2001; Siegel, 2001).
 is a polysonograph with the period of rapid eye movement (REM) highlighted. Chart (b) shows brainwaves at various stages of sleep, with the “awake” stage highlighted to show its similarity to the wave pattern of “REM” in chart (a).")
If people are deprived of REM sleep and then allowed to sleep without disturbance, they will spend more time in REM sleep in what would appear to be an effort to recoup the lost time in REM. This is known as the REM rebound, and it suggests that REM sleep is also homeostatically regulated. Aside from the role that REM sleep may play in processes related to learning and memory, REM sleep may also be involved in emotional processing and regulation. In such instances, REM rebound may actually represent an adaptive response to stress in non-depressed individuals by suppressing the emotional salience of aversive events that occurred in wakefulness (Suchecki, Tiba, & Machado, 2012). Sleep deprivation in general is associated with a number of negative consequences (Brown, 2012). The hypnogram below (Figure SC.15) shows a person’s passage through the stages of sleep.
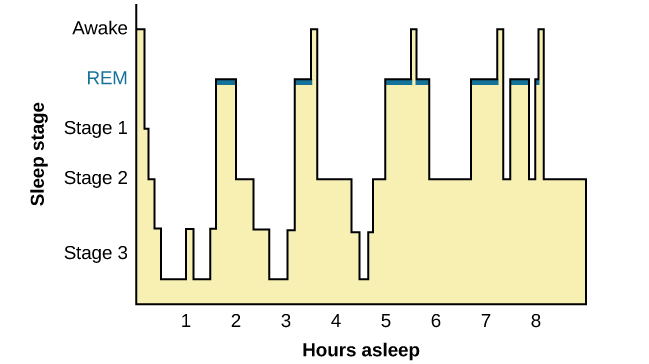
This is a hypnogram showing the transitions of the sleep cycle during a typical eight hour period of sleep. Table SC.2 explains what brain waves and behaviours we might be seeing with this hypnogram.
| Time of Night | Stage of Sleep | Type of Sleep | Experiences | Type of Brain Wave | Physical Signs or Behaviours |
|---|---|---|---|---|---|
| 10pm-11pm | N1 to N2 | Transition to Light Sleep | Dom starts to fall asleep, transitioning from light dozing to a more stable light sleep. | Theta waves | Slow rolling eye movements, reduced muscle activity |
| 11pm-12am | N3 | Deep Sleep | Dom enters deep sleep, crucial for physical restoration and memory consolidation. | Delta waves | Minimal movement, deep breathing |
| 12am-12:30am | N3 to REM | Deep to REM Sleep | Transition from deep sleep to the first REM period, marked by vivid dreams. | Mixed frequency brain waves transitioning to REM-specific waves | From minimal movement to rapid eye movements and muscle atonia (paralysis) |
| 12:30 a.m. – 1:00 a.m. | REM | REM Sleep | Dom experiences intense dreaming as brain activity increases; body remains immobile to prevent acting out dreams. | Mixed frequency brain waves | Rapid eye movements, muscle paralysis (REM atonia) |
| 1am-130am | Awake | Brief Awakening | Dom briefly wakes up, possibly due to disturbances or the end of a sleep cycle. | Alpha and beta waves | Possible turning or adjusting in bed, brief eye opening |
| 1:30 a.m. – 2:30 a.m. | N2 to REM | Light to REM Sleep | After falling back asleep, Dom quickly enters REM sleep, experiencing more vivid dreams. | Theta waves transitioning to mixed frequency brain waves | Sleep spindles and K complexes, followed by rapid eye movements and REM atonia |
| 2:30 a.m. – 3:00 a.m. | REM to Awake | REM to Brief Awakening | Ends REM sleep with a brief awakening, similar to the earlier pattern. | Mixed frequency brain waves to alpha and beta waves | Rapid eye movements, brief muscle activity upon waking |
| 3:00 a.m. – 4:00 a.m. | N2 to REM | Light to REM Sleep | Dom cycles back into light sleep and then into another REM period, with dreams becoming more fragmented. | Theta waves transitioning to mixed frequency brain waves | Sleep spindles and K complexes, followed by rapid eye movements and REM atonia |
| 4am-6am | N2, Awake, REM | Fluctuating Sleep Stages | The cycle of light sleep, brief awakenings, and REM sleep repeats with shortening intervals until Dom fully awakens at 6:00 AM. | Theta waves, alpha and beta waves during awake periods | Varying physical signs including sleep spindles, brief muscle activity during awakenings, and rapid eye movements in REM |
Sleep Problems and Disorders
Many people experience disturbances in their sleep at some point in their lives. Depending on the population and sleep disorder being studied, between 30 percent and 50 percent of the population suffer from a sleep disorder at some point in their lives (Bixler, Kales, Soldatos, Kaels, & Healey, 1979; Hossain & Shapiro, 2002; Ohayon, 1997, 2002; Ohayon & Roth, 2002). This section will describe several sleep disorders as well as some of their treatment options.
Insomnia
Insomnia, a consistent difficulty in falling or staying asleep, is the most common of the sleep disorders. Individuals with insomnia often experience long delays between the times that they go to bed and when they actually fall asleep. In addition, these individuals may wake up several times during the night, only to find that they have difficulty getting back to sleep. One of the criteria for insomnia involves experiencing these symptoms for at least three nights a week for at least one month’s time (Roth, 2007).
There are many reasons why people, and students in particular, might find it hard to sleep. Feeling stressed, anxious, or depressed can make it difficult to fall asleep or stay asleep (Albasheer et al., 2020). Also, habits like using social media or other electronic devices before bed can disrupt sleep (Abdalqader et al., 2018). This is because of the effects of blue light on the brain, which are discussed later on in this section.
Sleep hygiene is important. This means having good sleep habits, like a quiet, dark place to sleep and a regular bedtime. Poor sleep hygiene can lead to insomnia. The prevalence of students with symptoms of insomnia was high (39.7%; Carrión-Pantoja et al., 2022). Sometimes, students worry a lot at bedtime. This worry, or cognitive arousal, can keep them awake (Lethbridge & Pidgeon, 2017). Other factors, like headaches or feeling unhappy with life, can also affect students’ sleep (Angelone et al., 2011).
In short, many things can cause insomnia in university students. It’s not just about feeling stressed or anxious. It’s also about their habits, like using phones at night, and their overall health and happiness. Understanding these causes can help find ways to improve sleep for students.
“What causes insomnia? – Dan Kwartler” video by TED-Ed is licensed under the Standard YouTube licence.
Watch this video: SLEEP HYGIENE – ITS IMPORTANCE & METHODS TO PRACTICE GOOD SLEEP HYGIENE (10.5 minutes)
“SLEEP HYGIENE – ITS IMPORTANCE & METHODS TO PRACTICE GOOD SLEEP HYGIENE” video by MEDSimplified is licensed under the Standard YouTube licence.
Parasomnias
A parasomnia is one of a group of sleep disorders in which unwanted, disruptive motor activity and/or experiences during sleep play a role. Parasomnias can occur in either REM or NREM phases of sleep. Sleepwalking, restless leg syndrome, and night terrors are all examples of parasomnias (Mahowald & Schenck, 2000).
Sleepwalking
In sleepwalking, or somnambulism, the sleeper engages in relatively complex behaviours ranging from wandering about to driving an automobile. Sleepwalking most often occurs during slow-wave sleep, but it can occur at any time during a sleep period in some affected individuals (Mahowald & Schenck, 2000).
Restless leg syndrome
A person with restless leg syndrome (RLS) has uncomfortable sensations in the legs during periods of inactivity or when trying to fall asleep. Restless leg syndrome is quite common. The main reasons for RLS are not completely known, but it seems to involve both genes and the environment. Two important factors are not having enough iron in the body and problems with dopamine, a chemical in the brain (Connor et al., 2017; Earley et al., 2017).
Restless leg syndrome can sometimes be reduced with changes in daily habits or in some cases with drugs. Changing daily habits is an important start to treatment. This includes getting regular exercise and improving sleep hygiene to gain more hours and better quality of sleep. Caffeine and alcohol can make RLS worse and should be avoided (Ryan & Slevin, 2007).
Night terrors
Night terrors, also known as sleep terrors, are distressing episodes characterised by screaming, intense fear, and flailing while still asleep, often accompanied by sleepwalking (Mahowald & Schenck, 2000). Although individuals suffering from night terrors appear to be awake, they generally have no memories of the events that occurred, and attempts to console them are ineffective. Typically, individuals suffering from night terrors will fall back asleep again within a short time. Generally, treatment for night terrors is unnecessary unless there is some underlying medical or psychological condition that is contributing to the night terrors (Mayo Clinic, n.d.)
Sleep apnea
Recent studies have found that snoring and sleep apnea significantly impact sleep quality. Snoring is often a symptom of sleep apnea syndrome, a condition where breathing intermittently stops and starts during sleep, leading to reduced blood oxygen levels and serious health complications (Lu et al., 2009).
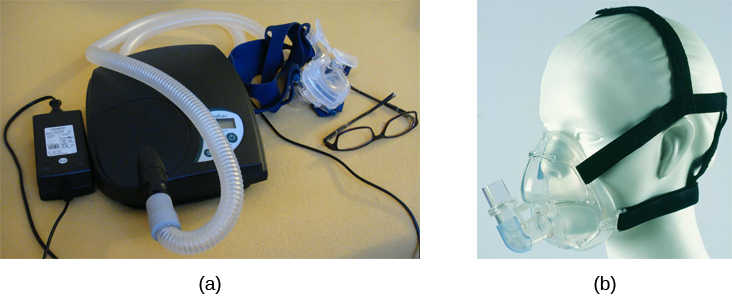
Sleep apnea is characterised by episodes where a sleeper’s breathing stops, often associated with brief periods of lighter sleep or wakefulness (Henry & Rosenthal, 2013). Sleep apnea is more common in individuals who are over a healthy weight, and is frequently associated with loud snoring. Treatments for sleep apnea include the use of continuous positive airway pressure (CPAP) devices, which have proven effective for mild to severe cases (McDaid et al., 2009).
Parasomnia summary
In summary, parasomnias are a category of sleep disorders characterised by unwanted behaviours or experiences during sleep, affecting individuals during both REM and NREM sleep phases. Common types include sleepwalking, where individuals might perform complex activities like walking or driving, often without any memory of the event. Restless Leg Syndrome (RLS) involves uncomfortable leg sensations and an irresistible urge to move the legs, impacting the ability to fall asleep. Night terrors, marked by intense fear and screaming, occur without the sufferer’s awareness. These disorders, while disruptive, can often be managed with treatments ranging from medication to lifestyle changes, depending on the severity and underlying causes.
Watch this video: Parasomnias Overview (.5 minutes)
“Parasomnias Overview” video by A Path To Better Sleep is licensed under the Standard YouTube licence.
Summary: Sleep Problems and Disorders
Section 4 provides an in-depth look at sleep, its essential functions, and the common disorders that disrupt it. It begins by defining sleep and exploring the reasons why sleep is crucial for our health, particularly its role in cognitive function. The section then outlines the stages of sleep, including NREM (Non-Rapid Eye Movement) stages and REM (Rapid Eye Movement) sleep, detailing the characteristics and importance of each stage for restorative rest.
The discussion extends to sleep problems and disorders, highlighting insomnia and parasomnias such as sleepwalking, restless leg syndrome, and night terrors. It emphasises the impact of these conditions on individuals’ well-being and the importance of managing them effectively. Sleep apnea is also covered, underscoring its potential health implications.
The section concludes with a summary of parasomnias and a case study presented as a fill-in-the-blank study game, designed to reinforce understanding of sleep disorders in an interactive manner.
Image Attributions
Figure SC.8. Photo by RDNE Stock project is used under the Pexels Content License.
Figure SC.9. Figure 4.6 as found in Psychology 2e by OpenStax is licensed under a CC BY 4.0 License.
Figure SC.10. Figure 4.7 as found in Psychology 2e by OpenStax is licensed under a CC BY 4.0 License. It is a derivative of “Perchance” by Ryan Vaarsi, which is licensed under a CC BY 2.0 license.
Figure SC.11. Figure 4.8 as found in Psychology 2e by OpenStax is licensed under a CC BY 4.0 License.
Figure SC.12. Figure 4.9 as found in Psychology 2e by OpenStax is licensed under a CC BY 4.0 License.
Figure SC.13. Figure 4.10 as found in Psychology 2e by OpenStax is licensed under a CC BY 4.0 License.
Figure SC.14. Figure 4.11 as found in Psychology 2e by OpenStax is licensed under a CC BY 4.0 License.
Figure SC.15. Figure 4.12 as found in Psychology 2e by OpenStax is licensed under a CC BY 4.0 License.
Figure SC.16. Figure 5.5 as found in Psychology 2e by OpenStax is licensed under a CC BY 4.0 License.
To calculate this time, we used a reading speed of 150 words per minute and then added extra time to account for images and videos. This is just to give you a rough idea of the length of the chapter section. How long it will take you to engage with this chapter will vary greatly depending on all sorts of things (the complexity of the content, your ability to focus, etc).
