- “SLUDGE”
Mnemonic for the effects of anticholinergics: Salivation decreased; Lacrimation decreased; Urinary retention; Drowsiness/dizziness; GI upset; Eyes (blurred vision/dry eyes).
- A1C
A lab test used to assess long-term blood glucose levels over 3 months. The general A1C target level is less than 7%.
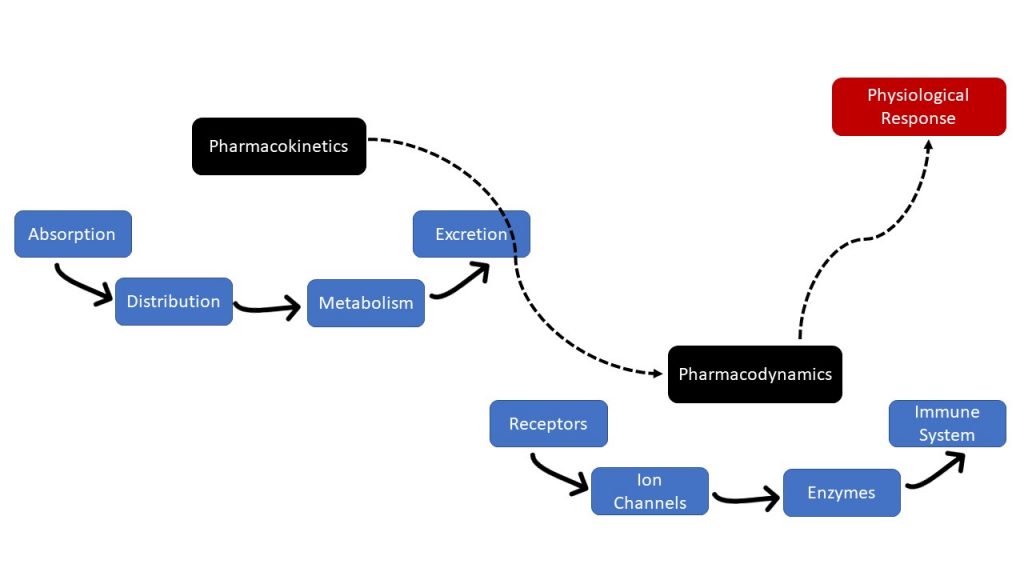
- absorption
The first stage of pharmacokinetics: medications enter the body and travel from the site of administration into the body's circulation.
- Accreditation Canada
is a national organization that accredits and certifies health care organizations in Canada.
- acetylcholine (ACh)
Binds to both nicotinic receptors and muscarinic receptors in the PNS.
- action potential
A change in voltage of a cell membrane in response to a stimulus that results in transmission of an electrical signal; unique to neurons and muscle fibers.
- acute dystonia
Painful muscle spasms.
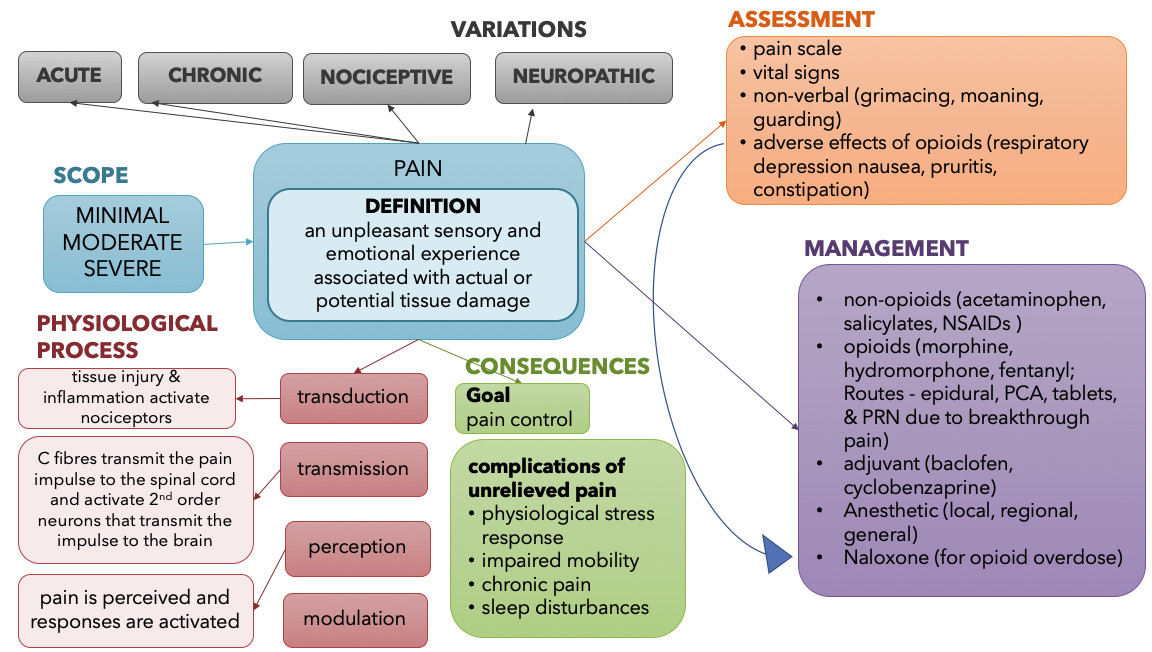
- acute pain
Pain that usually starts suddenly and has a known cause, like an injury or surgery. It normally gets better as your body heals and lasts less than three months.
- adjuvant analgesics
Drugs with a primary indication other than pain that have analgesic properties in some painful conditions. The group includes numerous drugs in diverse classes such as gabapentin (an anticonvulsant) or amitriptyline (a tricyclic antidepressant).
- adrenal medulla
Neuroendocrine tissue composed of postganglionic sympathetic nervous system (SNS) neurons that are stimulated by the autonomic nervous system to secrete hormones epinephrine and norepinephrine.
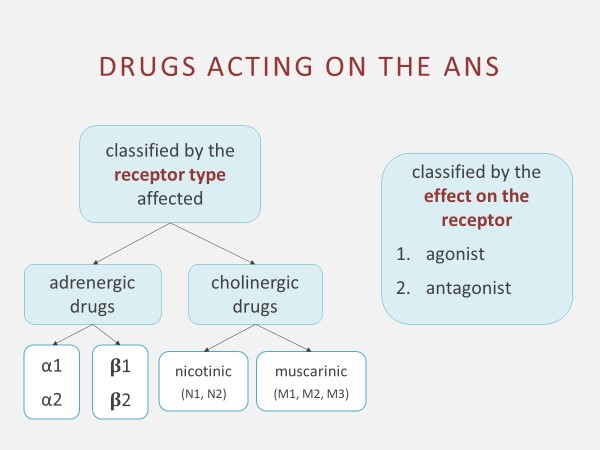
- adrenergic
Postganglionic neuron where neurotransmitters norepinephrine and epinephrine are released. Includes alpha (α) receptors and beta (β) receptors.
- adrenergic agonists
Mimic the effects of the body’s natural SNS stimulation on alpha (α) and beta (β) receptors. Also called sympathomimetics.
- adrenergic antagonists
Block the effects of the SNS receptors.
- adsorption
The adhesion of molecules to a surface. For example, bismuth salicylate coats the walls of the GI tract and binds the causative bacteria or toxin for elimination from the GI tract through the stool.
- adverse effects
An unintended pharmacological effect that occurs when a medication is administered correctly.
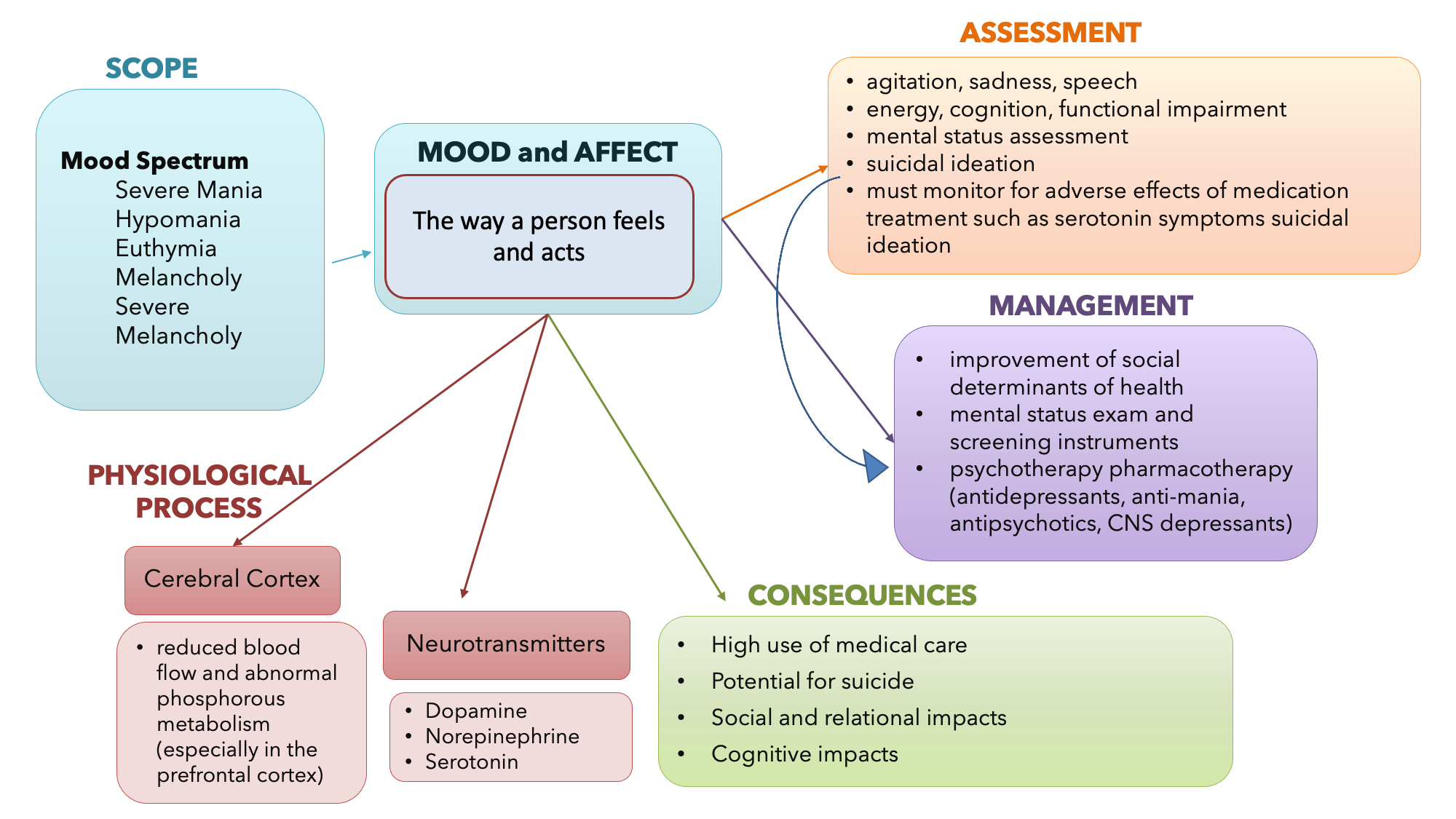
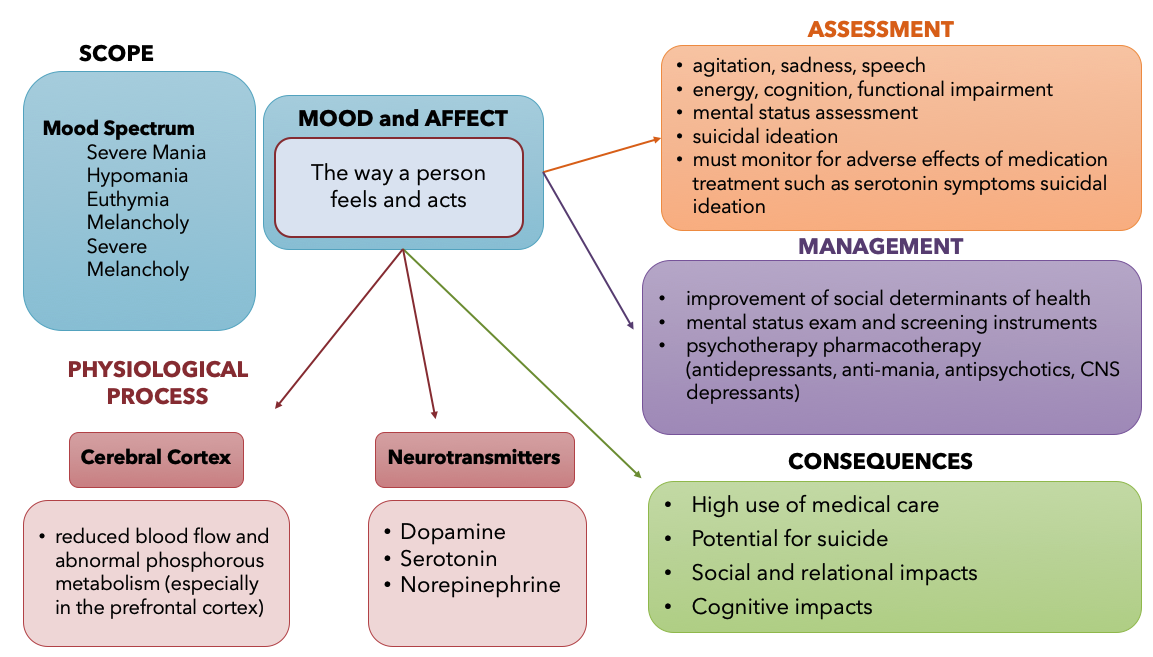
- affect
the observable response a person has to his or her own feelings,
- affinity
The strength of binding between drug and receptor.
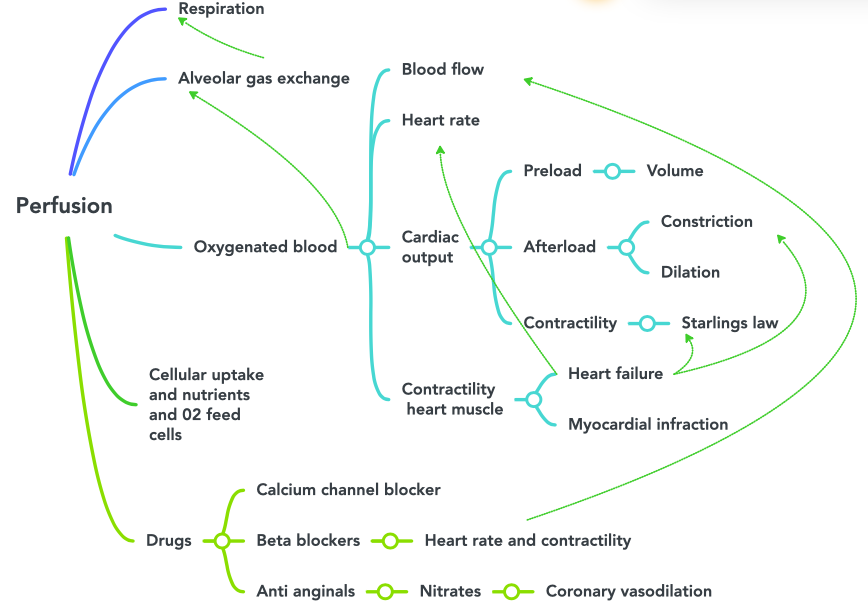
- afterload
The tension that the ventricles must develop to pump blood effectively against the resistance in the vascular system.
- agonist
A drug which binds to its "receptor" and produces its characteristic effect.
- akathisia
Distressing motor restlessness.
- aldosterone
A mineralocorticoid, released by the adrenal cortex, that controls fluid and electrolyte balance through the regulation of sodium and potassium.
- allergies
Allergies occur when the immune system reacts to a foreign substance and makes antibodies that identify a particular allergen as harmful, even though it isn't.
- ANA Standards of Professional Performance
Describe a competent level of behavior in the professional role, including activities related to ethics, culturally congruent practice, communication, collaboration, leadership, education, evidence-based practice, and quality of practice as defined by the American Nursing Association.
- anaphylaxis
A severe, potentially life-threatening allergic reaction. It can occur within seconds or minutes of exposure to something you're allergic to, such as peanuts or bee stings.
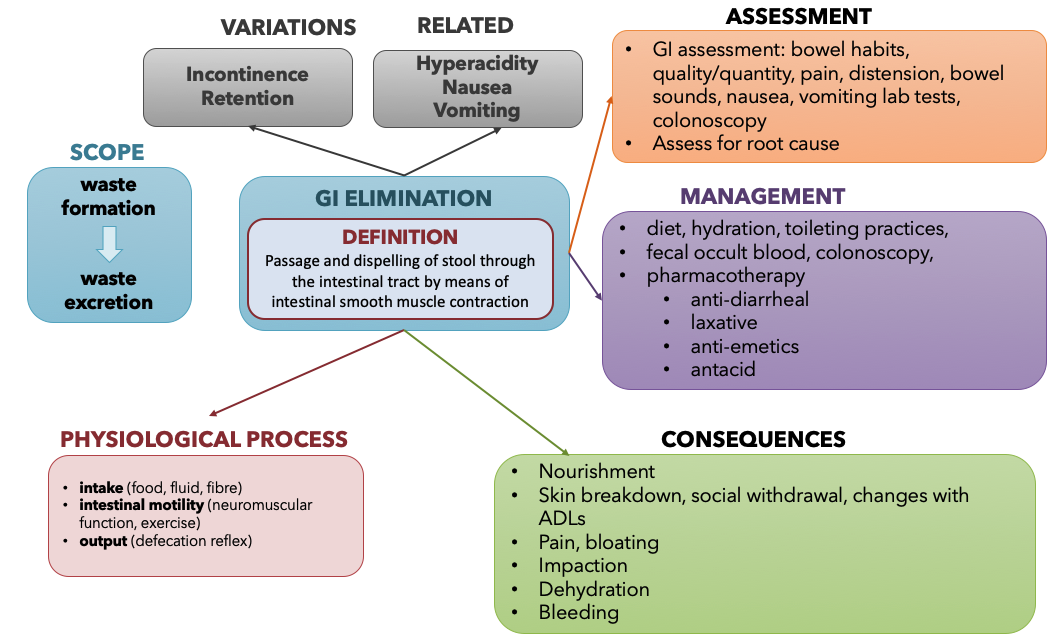
- antacids
Used to neutralize stomach acid and reduce the symptoms of heartburn.
- antagonist
A molecule that prevents the action of other molecules, often by competing for a cellular receptor; opposite of agonist.
- antagonistic interactions
Concurrent administration of two drugs causes harmful effects such as a decrease of drug activity, decreased therapeutic levels due to increased metabolism and elimination, or increased potential for toxicity due to decreased metabolism and elimination. An example of an antagonistic interaction is taking antacids with antibiotics, causing decreased absorption of the antibiotic.
- anticholinergics
Inhibit acetylcholine (ACh) which allows the SNS to dominate. Also called parasympatholytics or muscarinic antagonists. Overall use is to relax smooth muscle.
- anticoagulant
Any substance that opposes coagulation.
- antidiarrheals
Relieve the symptoms of diarrhea, such as an increased frequency and urgency when passing stools, but do not eliminate the cause of it.
- antidiuretic hormone (ADH)
ADH is released by the posterior pituitary in response to stimuli from osmoreceptors indicating high blood osmolarity. Its effect is to cause increased water reabsorption by the kidneys. As more water is reabsorbed by the kidneys, the greater the amount of water that is returned to the blood, thus causing a decrease in blood osmolarity. ADH is also known as vasopressin because, in very high concentrations, it causes constriction of blood vessels, which increases blood pressure by increasing peripheral resistance.
- antifungal
Medications that are used to treat fungal infections. For example, nystatin is used to treat Candida Albicans, a fungal infection.
- antimotility medications
Medications that help to treat diarrhea by slowing peristalsis.
- antiviral
Medications used to treat viral infections. For example, Tamiflu is used to treat influenza.
- anxiety
an alert to the human condition of impending doom, either real or imagined, and is accompanied by autonomic responses that serve as protective .
- area postrema
A structure in the medulla oblongata in the brainstem that controls vomiting. Its location in the brain also allows it to play a vital role in the control of autonomic functions by the central nervous system.
- arrhythmia
A deviation from the normal pattern of impulse conduction and contraction of the heart, which if serious and untreated, can lead to decreased cardiac output and death.
- arteriosclerosis
A condition when compliance in an artery is reduced and pressure and resistance within the vessel increase. This is a leading cause of hypertension and coronary heart disease, as it causes the heart to work harder to generate a pressure great enough to overcome the resistance.
- artery
A blood vessel that carries blood away from the heart (except for pulmonary arteries that carry oxygenated blood from the lungs back to the heart).
- atherosclerosis
A buildup, called plaque, that can narrow arteries enough to impair blood flow.
- autonomic nervous system
Controls cardiac and smooth muscle, as well as glandular tissue; associated with involuntary responses.
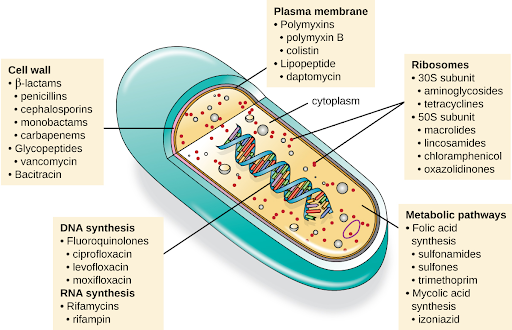
- bactericidal
Antimicrobial drugs that kill their target bacteria.
- bacteriostatic
Antimicrobial drugs that cause bacteria to stop reproducing but may not ultimately kill the bacteria.
- basal insulin
Long-acting (insulin glargine or insulin detemir) or intermediate-acting (NPH) insulin.
- beneficence
To “do good”.
- bioavailability
The ability of a drug or other chemical to be taken up by the body and made available in the tissue where it is needed.
- black box warnings
The strongest warnings issued by the Federal Drug Association (FDA) that signify a drug carries a significant risk of serious or life-threatening adverse effects.
- blood osmolarity
The concentration of solutes (such as sodium and glucose) in the blood.
- blood pressure
A type of hydrostatic pressure, or the force exerted by blood on the walls of the blood vessels or the chambers of the heart.
- blood-brain barrier
A nearly impenetrable barricade that is built from a tightly woven mesh of capillaries cemented together to protect the brain from potentially dangerous substances such as poisons or viruses.
- bradykinesia
Slowness in initiation and execution of voluntary movements.
- British Columbia College of Nurses and Midwives
The regulating body for nurses in British Columbia
- broad-spectrum antimicrobial
An antibiotic that targets a wide variety of bacterial pathogens, including both gram-positive and gram-negative species.
- Canadian Nurses Association (CNA)
A professional organization that represents the national and global interests of Canadian nurses.
- capillaries
Smallest arteries where nutrients and wastes are exchanged at the cellular level.
- cardiac output (CO)
A measurement of the amount of blood pumped by each ventricle in one minute.To calculate this value, multiply stroke volume (SV), the amount of blood pumped by each ventricle, by heart rate (HR), in contractions per minute (or beats per minute, bpm). It can be represented mathematically by the following equation: CO = HR × SV.
- catecholamines
Include norepinephrine, epinephrine and dopamine. Stimulate the adrenergic receptors.
- central nervous system (CNS)
Anatomical division of the nervous system located within the cranial and vertebral cavities, namely the brain and spinal cord.
- cerebrovascular accident (CVA)
Lack of blood flow to the brain that can cause irreversible brain damage, often referred to as a “stroke”.
- chemical synapse
Connection between two neurons, or between a neuron and its target, where a neurotransmitter diffuses across a very short distance.
- chemoreceptor trigger zone (CTZ)
Area in the brain that responds directly to toxins in the bloodstream and stimulates the vomiting center. The CTZ receives stimuli from several other locations in the body.
- chief cells
Cells that secret pepsinogen.
- cholinergic
Postganglionic neuron where acetylcholine (ACh) is released that stimulates nicotinic receptors and muscarinic receptors. Also relating to drugs that inhibit, enhance, or mimic the action of ACh.
- Chronic pain
Pain that lasts 6 months or more and can be caused by a disease or condition, injury, medical treatment, inflammation, or an unknown reason.
- chronotropic
Drugs may change the heart rate and rhythm by affecting the electrical conduction system of the heart and the nerves that influence it, such as by changing the rhythm (increasing) produced by the sinoatrial node. Positive chronotropes increase heart rate; negative chronotropes decrease heart rate.
- clients
Individual consumer of healthcare services who can be either a patient, resident or tenant
- clinical reasoning
A way that we think and process our knowledge including what we have read or learned in the past and apply it to the current practice context of what we are seeing right now.
- clostridium difficile (C diff)
Clostridium difficile causes pseudomembranous colitis, a superinfection that can be caused by broad spectrum antibiotic therapy.
- coagulation
The formation of a blood clot.
- Code of Ethics for Registered Nurses
Developed by the CNA as a guide for carrying out nursing responsibilities in a manner consistent with quality in nursing care and the ethical obligations of the profession.
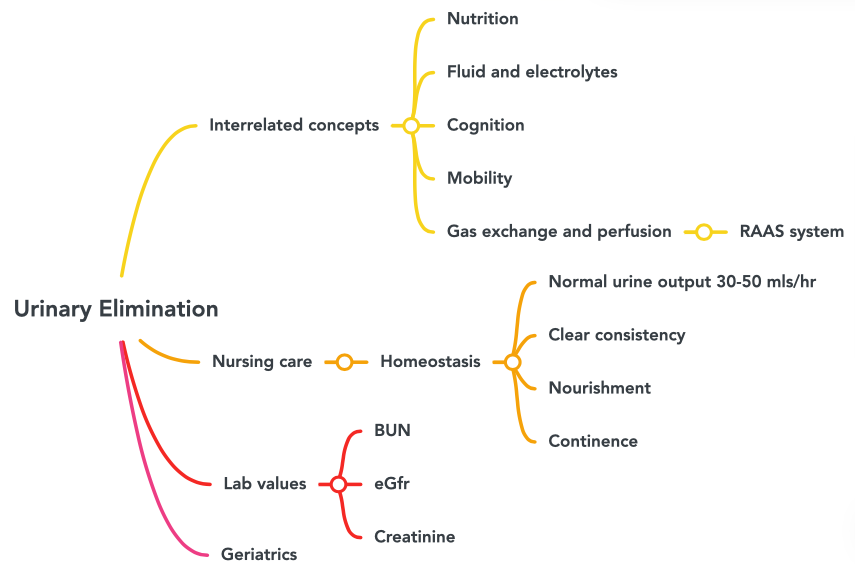
- cognition
the process of thought that embodies perception, attention, visuospatial cognition, language, learning, memory, and executive function with the higher order thinking skills of comprehension, insight, problem solving, reasoning, decision making, creativity, and metacognition
- compliance
The ability of any compartment to expand to accommodate increased content. The greater the compliance of an artery, the more effectively it is able to expand to accommodate surges in blood flow without increased resistance or blood pressure. Veins are more compliant than arteries and can expand to hold more blood. When vascular disease causes stiffening of arteries, compliance is reduced and resistance to blood flow is increased.
- constipation
Three or fewer bowel movements in a week; stools that are hard, dry or lumpy; stools that are difficult or painful to pass; or the feeling that not all stool has passed.
- contractility
The force of contraction of the heart.
- controls on practice
Explains the bases for nurses' scope of practice. There are four levels of controls on registered nurses' practice.
- cultural competence
The process by which nurses demonstrate culturally congruent practice.
- cultural safety
Outcome-based respectful engagement that addresses power imbalances from a societal and health care systems lens.
- culturally congruent practice
The application of evidence-based nursing that is in agreement with the preferred cultural values, beliefs, worldview, and practices of the healthcare consumer and other stakeholders.
- culture
A test performed to examine different body substances for the presence of bacteria or fungus.
- cyanotic
A bluish or purplish discoloration (as of skin) due to deficient oxygenation of the blood.
- cytochrome P-450 enzymes
Enzymes produced from the cytochrome P450 genes involved in the formation (synthesis) and breakdown (metabolism) of various molecules, chemicals, and medications within cells.
- defecation
The digestive process where undigested materials are removed from the body as feces.
- diabetes insipidus (DI)
A disease characterized by underproduction of ADH that causes chronic dehydration.
- diarrhea
The passage of three or more loose or liquid stools per day (or more frequent passage than is normal for the individual).
- diastole
The period of relaxation that occurs as the chambers of the heart fill with blood.
- distribution
The second stage of pharmacokinetics; the process by which medication is distributed throughout the body.
- do not crush list
A list of medications that should not be crushed, often due to a sustained-release formulation.
- dose-dependent
A more significant response occurs in the body when the medication is administered in large doses to provide a large amount of medication to the site of infection for a short period of time.
- dose-response
As the dose of a drug increases, the response should increase. The slope of the curve is characteristic of the particular drug-receptor interaction.
- dromotropic
Stimulation causes increases speed of conduction between SA and AV node.
- drug diversion
The transfer of any legally prescribed controlled substance from the individual for whom it was prescribed to another person for any illicit use.
- Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS)
Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS): A condition reported in patients taking antiepileptic drugs. Some of these events have been fatal or life-threatening. DRESS typically presents with fever, rash, lymphadenopathy, and/or facial swelling.
- Drugs
Medications or other substances that have a physiological effect when introduced to the body.
- duration
The length of time that a medication is available within the body and producing its desired therapeutic effect.
- dystonia
Inappropriate and continuous muscle contraction.
- edema
The presence of excess tissue fluid around the cells.
- efficacy
The maximum effect of which the drug is capable.
- electrical synapse
Connection between two neurons, or any two electrically active cells, where ions flow directly through channels spanning their adjacent cell membranes.
- embolus
When a portion of a thrombus breaks free from the vessel wall and enters the circulation. An embolus that is carried through the bloodstream can be large enough to block a vessel critical to a major organ. When it becomes trapped, an embolus is called an embolism. In the heart, brain, or lungs, an embolism may accordingly cause a heart attack, a stroke, or a pulmonary embolism.
- error-prone abbreviations
Abbreviations, symbols, and dose designations that are frequently misinterpreted and involved in harmful medication errors.
- excretion
The final stage of pharmacokinetics; process by which the body eliminates waste or excess.
- exocrine gland
Gland that secretes digestive enzymes.
Involuntary motor symptoms similar to those associated with Parkinson’s disease. Includes symptoms such as akathisia (distressing motor restlessness) and acute dystonia (painful muscle spasms.) Often treated with anticholinergic medications such as benztropine and trihexyphenidyl.
- fibrillation
An uncoordinated beating of the heart, which if serious and untreated, can lead to decreased cardiac output and death.
- fibrinolysis
The gradual degradation of a clot.
- fight-or-flight
The response when the SNS is stimulated causing the main effects of increased heart rate; increased blood pressure; and bronchodilation.
- fight-or-flight response
The response when the SNS is stimulated causing the main effects of increased heart rate; increased blood pressure; and bronchodilation.
- first pass effect
The breakdown of orally administered drugs in the liver and intestines.
- gait disturbance
An abnormal way of walking, such as shuffling feet.
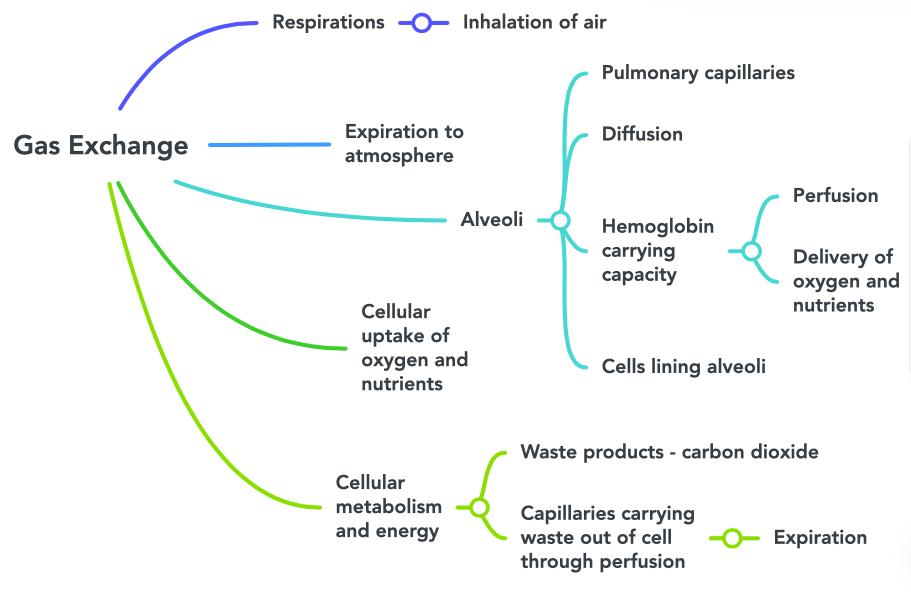
- gas exchange
The process at the alveoli level where blood is oxygenated and carbon dioxide, the waste product of cellular respiration, is removed from the body.
- gastroenteritis
Infection of the intestines.
- gastroesophageal reflux disease (GERD)
Caused by excessive hydrochloric acid that tends to back up, or reflux, into the lower esophagus.
- general adaptation syndrome (GAS)
The pattern in which the body responds in different ways to stress: The alarm reaction (otherwise known as the “fight or flight response,” the stage of resistance, and the stage of exhaustion).
- glycolysis
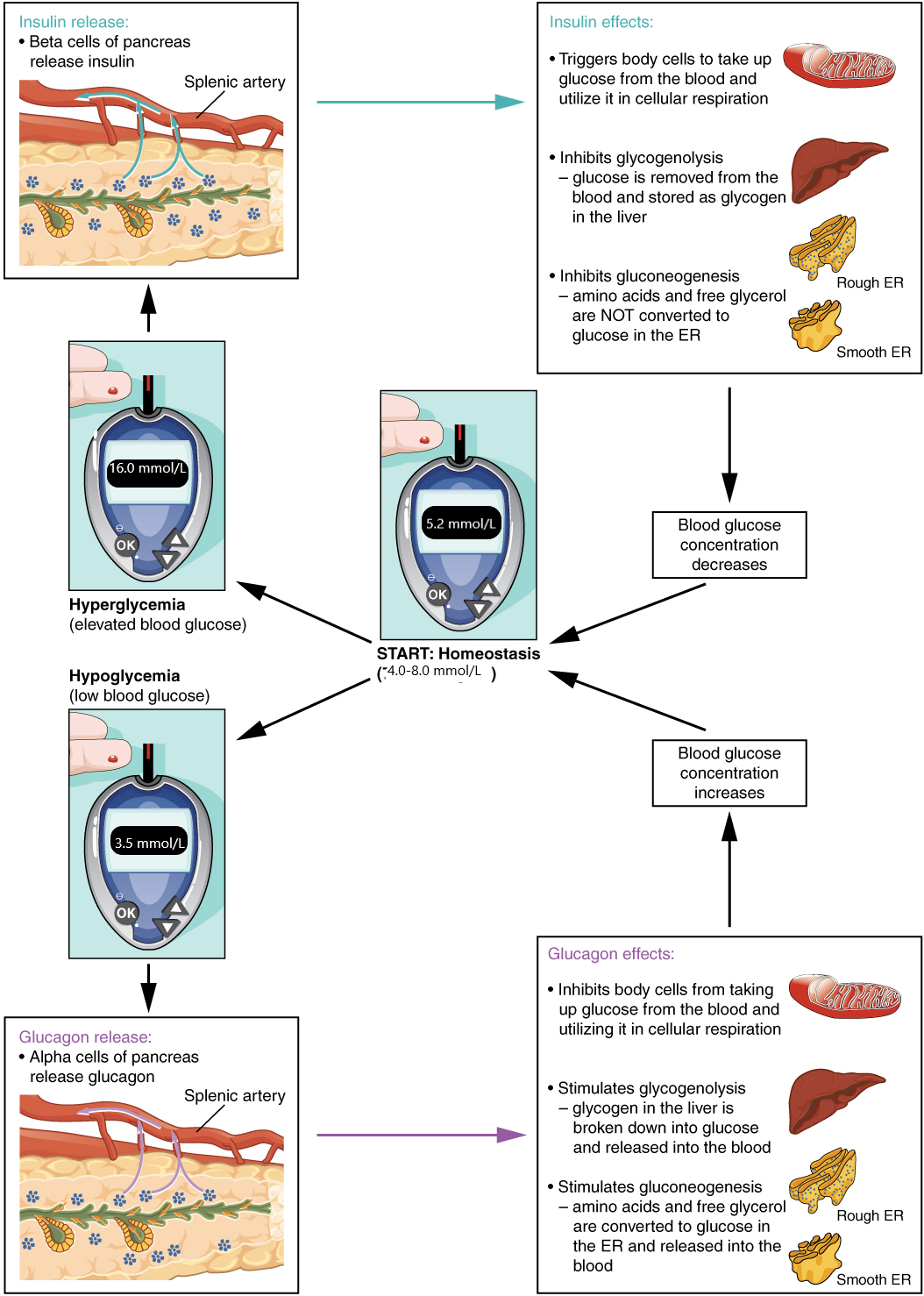
Stimulated by insulin, the metabolism of glucose for generation of ATP.
- glyconeogenesis
The breakdown of glycogen into glucose, causing elevated blood sugar.
- goiter
A visible enlargement of the thyroid gland when there is hyperstimulation of TSH due to deficient levels of T3 and T4 hormones in the bloodstream or an autoimmune reaction in which antibodies overstimulate the follicle cells of the thyroid gland, causing hyperthyroidism.
- gram + infection
Infections caused by Streptococcus and Staphylococcus bacteria are examples of gram + infection.
- Gram negative
Infections that often grow between aerobic and anaerobic areas.
- gram stain
A test used to quickly diagnose bacterial infection .Identification of bacteria as gram + or gram - assists the healthcare provider in selecting an appropriate antibiotic to treat the infection.
- half-life
The rate at which 50% of a drug is eliminated from the bloodstream.
- health literacy
The ability to access, understand, evaluate, and communicate information as a way to promote, maintain, and improve health in a variety of settings across the life course
- hematemesis
Blood in the vomit.
- hemostasis
The process by which the body temporarily seals a ruptured blood vessel and prevents further loss of blood.
- high-risk
Drugs that bear a heightened risk of causing significant patient harm when they are used in error.
- homeostasis
Balance between the SNS and PNS. At each target organ, dual innervation determines activity. For example, SNS stimulation causes the heart rate to increase, whereas PNS stimulation causes the heart rate to decrease.
- hormones
Chemical signals sent by the endocrine organs and transported via the bloodstream throughout the body where they bind to receptors on target cells and induce a characteristic response.
- humoral stimuli
Changes in blood levels of non-hormone chemicals that cause an endocrine gland to release or inhibit a hormone to maintain homeostasis. For example, high blood sugar causes the pancreas to release insulin.
- hypercalcemia
Elevated levels of calcium in the bloodstream.
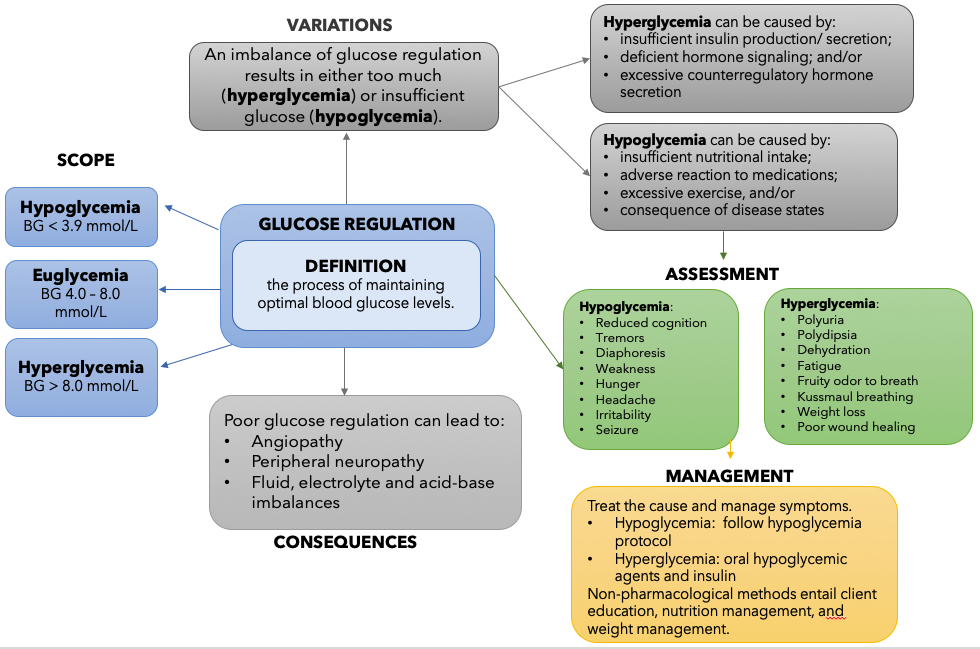
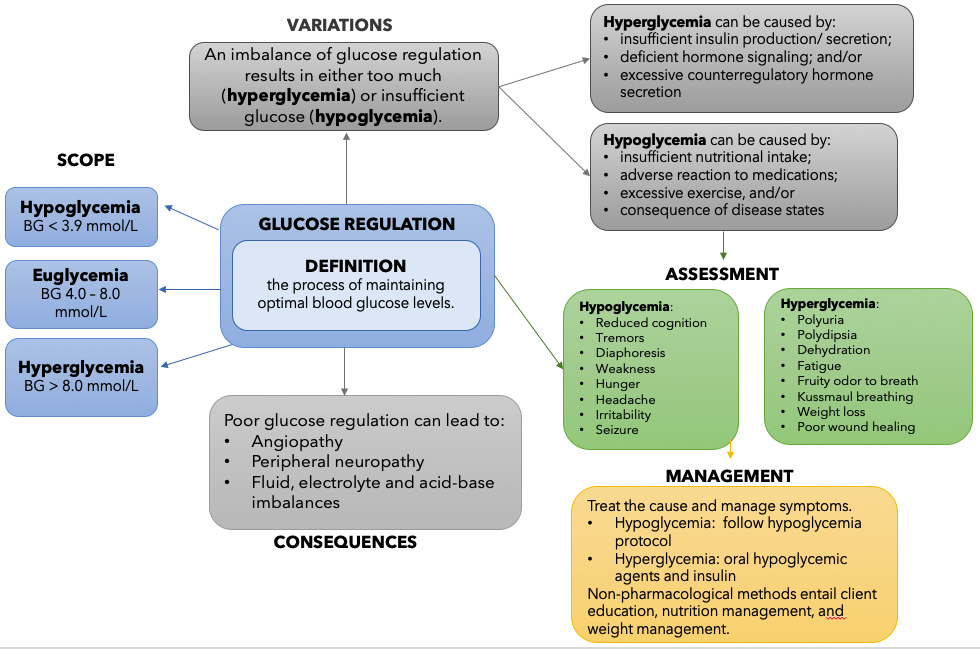
- hyperglycemia
Elevated blood sugar.
- hyperlipidemia
Elevated cholesterol levels in the blood that increase a patient’s risk for heart attack and stroke.
- hyperparathyroidism
A disorder caused by an overproduction of PTH that results in excessive calcium resorption from bone, causing significantly decreased bone density and spontaneous fractures, decreased responsiveness of the nervous system, and calcium deposits in the body’s tissues and organs, impairing their functioning.
- hypertension
Chronically elevated blood pressure.
- hypertensive crisis
Severe hypertension (blood pressure greater than 180/120 mm Hg) with evidence of organ dysfunction. Symptoms may include occipital headache (which may radiate frontally), palpitations, neck stiffness or soreness, nausea or vomiting, sweating, dilated pupils, photophobia, shortness of breath, or confusion. Either tachycardia or bradycardia may be present and may be associated with constricting chest pain. Seizures may also occur. Intracranial bleeding, sometimes fatal, has been reported in association with the increase in blood pressure.
- hyperthyroidism
Abnormally elevated blood level of thyroid hormones T3 and T4, often caused by a pituitary tumor, thyroid tumor, or autoimmune reaction in which antibodies overstimulate the follicle cells of the thyroid gland
- hypervolemia
Excessive fluid volume caused by retention of water and sodium, as seen in patients with heart failure, liver cirrhosis, and some forms of kidney disease.
- hypoglycemia
A blood glucose level below 70 mg/dL; severe hypoglycemia refers to a blood glucose level below 40.
- hypoparathyroidism
Abnormally low blood calcium levels caused by parathyroid hormone deficiency, which may develop following thyroid surgery. Low blood calcium can cause muscle twitching, cramping, spasms, or convulsions; severe deficits can paralyze muscles, including those involved in breathing, and can be fatal.
- hypothalamic-pituitary-adrenal (HPA) axis
The hypothalamus stimulates the release of ACTH from the pituitary, which then stimulates the adrenal cortex to produce the hormone cortisol and steroid hormones important for the regulation of the stress response, blood pressure and blood volume, nutrient uptake and storage, fluid and electrolyte balance, and inflammation.
- hypothalamus–pituitary complex
The “command center” of the endocrine system that secretes several hormones that directly produce responses in target tissues, as well as hormones that regulate the synthesis and secretion of hormones of other glands. In addition, the hypothalamus–pituitary complex coordinates the messages of the endocrine and nervous systems.
- hypothyroidism
Abnormally low blood levels of thyroid hormones T3 and T4 in the bloodstream.
- hypovolemia
Decreased blood volume that may be caused by bleeding, dehydration, vomiting, severe burns, or by diuretics used to treat hypertension. Treatment typically includes intravenous fluid replacement.
- immune-mediated disease process
Occurs when the body's immune system attacks the central nervous system.
- inappropriate polypharmacy
Present when one or more medicines are prescribed that are not or no longer needed.
- indications
The use of a drug for treating a particular condition or disease. The FDA determines if there is enough evidence for a labeled indication of a drug. Providers may also prescribe medications for off-label indications if there is reasonable scientific evidence that the drug is effective, but these uses have not been approved by the FDA.
- inotropic
Stimulation causes increased force of contraction.
- insulin
A hormone that facilitates the uptake of glucose into skeletal and adipose body cells.
- international normalized ratio
A blood test used to monitor the effects of warfarin and to achieve therapeutic range, generally between 2.0 and 3.5 based on the indication.
- intrinsic factor
Necessary for the absorption of vitamin B12 in the small intestine.
- involuntary responses
Responses that the brain controls without the need for conscious thought.
- ischemia
Reduced blood flow to the tissue region “downstream” of the narrowed vessel
- look-alike and sound-alike drugs
Medications that require special safeguards to reduce the risk of errors and minimize harm.
- loop of Henle
A component of the nephron where loop diuretics act to eliminate sodium and water
- maleficence
Causing harm to patients.
- mania
Periods of extreme highs in bipolar disorder. Manic episodes may include these symptoms rapid speech, hyperactivity, reduced need for sleep, flight of ideas, grandiosity, poor judgement, aggression/hostility, risky sexual behavior, neglected basic self-care, or decreased impulse control.
- mechanism of action
How a medication works at a cellular level within the body.
- metabolism
The breakdown of a drug molecule via enzymes in the liver (primarily) or intestines (secondarily).
- methicillin-resistant S. aureus (MRSA)
An infection caused by Methicillin-resistant Staphylococcus aureus that is difficult to treat because it exhibits resistance to nearly all available antibiotics.
- mineralocorticoids
Hormones released by the adrenal cortex that regulate body minerals, especially sodium and potassium, that are essential for fluid and electrolyte balance. Aldosterone is the major mineralocorticoid.
- misuse
The use of illegal drugs and/or the use of prescription drugs in a manner other than as directed by a doctor, such as use in greater amounts, more often, or longer than told to take a drug or using someone else’s prescription.
- mobility
Refers to purposeful physical movement, including gross simple movements, fine complex movements, and coordination; "State or quality of being mobile or movable."
- mood
the way a person feels .
- motor neurons
Consist of the somatic nervous system that stimulates voluntary movement of muscles, and the autonomic nervous system that controls involuntary responses.
- muscarinic agonists
Also called parasympathomimetics. Primarily cause smooth muscle contraction, resulting in decreased HR, bronchoconstriction, increased GI/GU tone, and pupil constriction.
- muscle spasticity
Condition in which certain muscles are continuously contracted. This contraction causes stiffness or tightness of the muscles and can interfere with normal movement, speech, and gait. Spasticity is usually caused by damage to the portion of the brain or spinal cord that controls voluntary movement.
- myocardial infarction
Commonly referred to as a heart attack, resulting from a lack of blood flow (ischemia) and oxygen to a region of the heart, resulting in death of the cardiac muscle cells.
- narrow-spectrum antimicrobial
An antibiotic that targets only specific subsets of bacterial pathogens.
- National Patient Safety Goals
Goals established by the Joint Commission to help accredited organizations address specific areas of concern related to patient safety.
- negative feedback loop
Characterized by the inhibition of further secretion of a hormone in response to adequate levels of that hormone.
- negative inotropic factors
Factors that decrease contractility.
- nerve
Cord-like bundle of axons located in the peripheral nervous system that transmits sensory input and response output to and from the central nervous system.
- neural stimuli
Released in response to stimuli from the nervous system. For example, the activation of the release of epinephrine and norepinephrine in the fight-or-flight response is stimulated by the sympathetic nervous system.
- neuroleptic malignant syndrome (NMS)
Potentially life-threatening adverse effect that includes high fever, unstable blood pressure, and myoglobinemia.
- neurons
Cells that carry electrical impulses to the synapse of a target organ.
- neurotransmitter
Chemical signal that is released from the synaptic end bulb of a neuron to cause a change in the target cell.
- nociceptors
Nerve endings that selectively respond to painful stimuli and send pain signals to the brain and spinal cord.
- non-pharmacologic therapy
Treatments that do not involve medications, including physical treatments (e.g., exercise therapy, weight loss) and behavioral treatments (e.g., cognitive behavioral therapy).
- nonselective beta blockers
Medications that block both Beta 1 and Beta 2 receptors, thus affecting both the heart and lungs.
- nursing
the application of professional nursing knowledge, skills, and judgment for the purpose of: (a) promoting, maintaining, and restoring health; (b) preventing illness, injury, or disability; (c) caring for persons who are sick, injured, disabled, or dying; (d) assisting in pre-natal care, childbirth, and postnatal care; (e) health teaching and health counselling; (f) coordinating health care; or (g) engaging in administration, teaching, or research.
- nursing process
Standards of Practice that include Assessment, Diagnosis, Outcome Identification, Planning, Implementation, and Evaluation components of providing patient care.
- onset
When a medication first begins to work and exerts a therapeutic effect.
- ophthalmoplegia
Weakness in eye muscles.
- orthostatic hypotension
A significant change in blood pressure from lying to sitting to standing.
- osmoreceptors
Specialized cells within the hypothalamus that are sensitive to the concentration of sodium ions and other solutes in the bloodstream.
- osmotic agents
Cause water to be retained with the stool, increasing the number of bowel movements and softening the stool so it is easier to pass.
- pain
an unpleasant sensory and emotional experience associated with actual or potential tissue damage
- pallor
A deficiency of color especially of the face: paleness.
- paradoxical effect
An effect that is opposite to what is expected.
- parasympathetic division (PNS)
Includes nerves outside the brain and spinal cord. Associated with the “rest and digest” response. Stimulation of PNS causes decreased heart rate, decreased blood pressure via vasodilation, bronchial constriction, and stimulates intestinal motility, salivation, and relaxation of the bladder.
- parasympathomimetics
Also called muscarinic agonists. Primarily cause smooth muscle contraction, resulting in decreased HR, bronchoconstriction, increased GI/GU tone, and pupil constriction.
- parathyroid hormone (PTH)
The hormone released by parathyroid glands; involved in the regulation of blood calcium levels.
- parietal cells
cells in the gastric glands that produce and secrete hydrochloric acid (HCl) and intrinsic factor
- partial thromboplastin time (PTT)
A blood test used to monitor how long it takes for a patient’s blood to clot. Used for patients receiving IV heparin therapy to achieve therapeutic range.
- pathogen
An organism causing disease to its host.
- patient controlled analgesia (PCA)
Patient-controlled analgesia (PCA) is a type of pain management that lets the client decide when to get a dose of pain medicine (typically an opioid). To receive the opioid, the patient pushes a button on the PCA device, which releases a specific dose but also has a lockout mechanism to prevent an overdose.
- peak
When the maximum concentration of drug is in the body.
- pepsin
A digestive enzyme.
- peptic ulcer disease (PUD)
Occurs when gastric or duodenal ulcers are caused by the breakdown of GI mucosa by pepsin in combination with the caustic effects of hydrochloric acid.
- perfusion
The ability of or heart to move oxygen and nutrients throughout the body to ensure cellular processes are able to function appropriately.
- peripheral nervous system (PNS)
An anatomical division of the nervous system that is largely outside the cranial and vertebral cavities, namely all parts except the brain and spinal cord.
- pharmacodynamics
The study of how drugs act at target sites of action in the body.
- pharmacogenetics
The study of how people's genes affect their response to medicines.
- pharmacokinetics
The study of how the body absorbs, distributes, metabolizes, and eliminates drugs.
- pharmacology
The science dealing with actions of drugs on the body.
- pharmacotherapeutics
The clinical purpose or reason for the medication
- pharmacy
The science of preparation of drugs.
- polypharmacy
The concurrent use of multiple medications.
- positive inotropic factors
Factors that increase contractility.
- postganglionic neurons
Postganglionic neurons of the autonomic system are classified as either cholinergic, meaning that acetylcholine (ACh) is released, or adrenergic, meaning that norepinephrine is released.
- postural instability
Abnormal fixation of posture (stoop when standing), problems with equilibrium, and righting reflex.
- potency
The drug dose required to produce a specific intensity of effect.
- practice standards
Guide and direct nurses' practice. They set out levels of performance that BCCNM nurse registrants are required to achieve in their practice.
- prandial insulins
During or relating to the eating of food.
- preganglionic neurons
All preganglionic neurons (in the SNS and PNS) release acetylcholine (ACh).
- preload
The amount of blood in the atria just prior to atrial contraction.
- prescription monitoring programs
Collects information about prescription and dispensing of controlled substances for the purposes of monitoring, analysis and education
- probiotics
Used for the prevention and treatment of diarrhea by restoring normal bacteria flora in the gastrointestinal tract.
- professional standards
Statements about levels of performance that nurses are required to achieve in their practice. They reflect the values of the nursing profession, clarify what the profession expects of nurses, and represent the criteria against which nurses’ practice in British Columbia is measured by clients, employers, colleagues, themselves and others
- prokinetic
Medications used to promote peristalsis to empty the gastrointestinal tract and reduce nausea.
- prostaglandins
Produced in nearly all cells and are part of the body’s way of dealing with injury and illness. Prostaglandins act as signals to control several different processes depending on the part of the body in which they are made. Prostaglandins are made at the sites of tissue damage or infection, where they cause inflammation, pain, and fever as part of the healing process.
- prothrombin time
A blood test used to monitor the effects of warfarin.
- proton pump inhibitor
Binds to the hydrogen-potassium ATPase enzyme system of the parietal cell and inhibit the release of hydrogen ions into the stomach.
- prototype
A common individual drug that represents a drug class or group of medications having similar chemical structures, mechanism of action and mode of action.
- rebound hyperacidity
A side effect of medication causing elevated levels of hydrochloric acid in the stomach after the medication is discontinued.
- registered nurse (RN)
An individual who is educationally prepared and licensed by province or territory to practice as a registered nurse.
- renin-angiotensin-aldosterone system
Specialized cells in the kidneys that respond to decreased blood flow by secreting renin into the blood. Renin converts the plasma protein angiotensinogen into its active form—angiotensin I. Angiotensin I circulates in the blood and is then converted into angiotensin II in the lungs. This reaction is catalyzed by the enzyme angiotensin-converting enzyme (ACE). Angiotensin II is a powerful vasoconstrictor, greatly increasing blood pressure. It also stimulates the release of ADH and aldosterone, a hormone produced by the adrenal cortex. Aldosterone increases the reabsorption of sodium into the blood by the kidneys causing reabsorption of water and increasing blood volume and raising blood pressure.
- resistance
A characteristic of bacteria demonstrating lack of effective treatment by an antibiotic when a sensitivity analysis is performed.
- respiratory rate
The total number of breaths, or respiratory cycles, that occur each minute. A child under 1 year of age has a normal respiratory rate between 30 and 60 breaths per minute, but by the time a child is about 10 years old, the normal rate is closer to 18 to 30. By adolescence, the normal respiratory rate is similar to that of adults, 12 to 18 breaths per minute.
- rigidity
Increase muscle tone and increase resistance to movement (Arms and Legs Stiff) – as severity increases cogwheel rigidity.
- root cause analysis
An analysis after an error occurs to help identify not only what and how an event occurred, but also why it happened. When investigators are able to determine why an event or failure occurred, they can create workable corrective measures that prevent future errors from occurring.
- safety culture
The culture of a health care agency that empowers staff to speak up about risks to patients and to report errors and near misses, all of which drive improvement in patient care and reduce the incidence of patient harm.
- scheduled medications
classification tool for drugs, substances, and certain chemicals that are used to make drugs. Defined by medical use, potential for misuse, and safety or dependence liability.
- selective beta blockers
Medications that mostly inhibit B1 receptors.
- selectivity
How readily the drug targets specific cells to produce an intended therapeutic effect.
- sensitivity analysis
A test performed in addition to a culture in order to select an effective antibiotic to treat the microorganism.
- sensory neurons
Sense the environment and conduct signals to the brain that become a conscious perception of that stimulus.
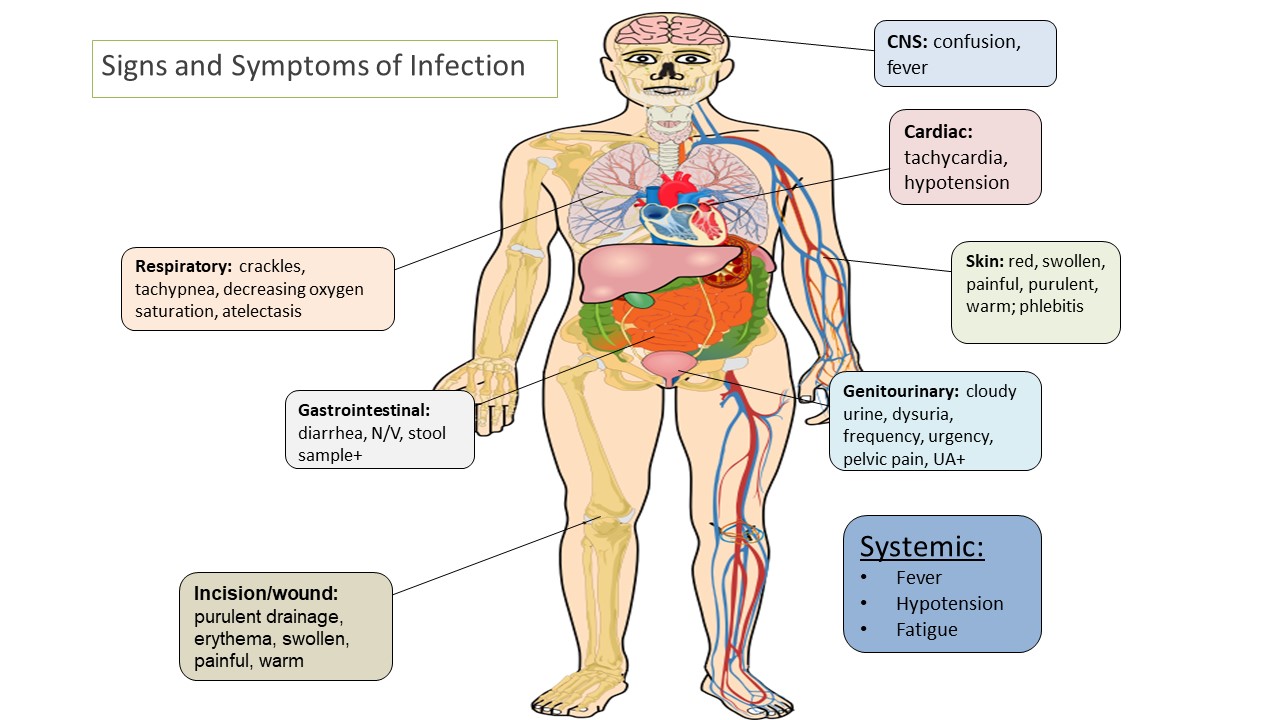
- sepsis
Sepsis is a life-threatening condition that arises when the body's response to infection causes injury to its own tissues and organs. It is defined as the presence of infection with at least 2 symptoms of systemic inflammatory response syndrome.
- serotonin syndrome
Symptoms associated with serotonin syndrome may include the following combination of signs and symptoms: mental status changes (e.g., agitation, hallucinations, delirium, and coma), autonomic instability (e.g., tachycardia, labile blood pressure, dizziness, diaphoresis, flushing, hyperthermia), neuromuscular symptoms (e.g., tremor, rigidity, myoclonus, hyperreflexia, incoordination), seizures, with or without gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea).
- side effect
The effect of a drug, other than the desired effect, sometimes in an organ other than the target organ.
- sinoatrial (SA) node.
Normal cardiac rhythm is established by the sinoatrial (SA) node. The SA node has the highest inherent rate of depolarization and is known as the pacemaker of the heart.
- sinus rhythm
Normal electrical pattern followed by contraction of the heart.
- social determinants of health
Poverty, education, safe medication, and other healthcare disparities that affect a patient’s health.
- social determinants of health SDOH
Poverty, education, safe medication, and other healthcare disparities that affect a patient’s health.
- somatic nervous system
Causes contraction of skeletal muscles; associated with voluntary responses.
- sputum
Matter expectorated from the respiratory system and especially the lungs that is composed of mucus but may contain pus, blood, fibrin, or microorganisms (such as bacteria) in diseased states.
- state nurse practice act
Laws enacted by state legislature setting professional standards of nursing care to which nurses are held accountable by the State Board of Nursing.
- state nurse practice acts
Laws enacted by state legislature setting professional standards of nursing care to which nurses are held accountable by the State Board of Nursing.
- status epilepticus
A state of repeated or continuous seizures.
- stimulants
Laxatives that cause the intestines to contract, inducing stool to move through the colon.
- stool softeners
Laxatives that facilitate movement of water and fats into stool to make it soft and improve regularity of bowel movements.
- stress ulcer prophylaxis
Medication to prevent the formation of stress ulcers.
- stress-related mucosal damage
A common condition in hospitalized patients that can lead to PUD.
- stroke volume (SV)
The amount of blood that both ventricles pump during each contraction, normally in the range of 70–80 mL.
- superinfection
A secondary infection in a patient having a preexisting infection. C diff and yeast infections as a result of antibiotic therapy are examples of superinfections.
- Surface epithelium cells
Cells found within the lining of the stomach that secrete mucus as a protective coating.
- sympathetic division (SNS)
Associated with the “fight or flight response.” Stimulation causes the main effects of increased heart rate, increased blood pressure via the constriction of blood vessels, and bronchodilation.
- sympathomimetics
Mimic the effects of the body’s natural SNS stimulation of adrenergic receptors. Also called adrenergic agonists.
- synapse
The connection between the neuron and its target cell.
- synergistic interaction
Concurrent drug administration producing a synergistic interaction that is better than the efficacy of either drug alone. An example of synergistic drug combinations is trimethoprim and sulfamethoxazole (Bactrim).
- systole
The period of contraction that the heart undergoes while it pumps blood into circulation.
- tardive dyskinesia
Involuntary contraction of the oral and facial muscles (such as tongue thrusting) and wavelike movements of the extremities.
- thalamus
The region of the central nervous system that acts as a relay for sensory pathways.
- THC
Tetrahydrocannabinoids found in marijuana.
- therapeutic index
A measurement of the amount of drug that produces a therapeutic effect compared to the amount of drug that produces a toxic effect.
- therapeutic window
The dosing window in which the safest and most effective treatment will occur.
- threshold
The membrane voltage at which an action potential is initiated.
- thrombus
An aggregation of platelets, erythrocytes, and WBCs trapped within a mass of fibrin strands that adhere to the vessel wall and decrease the flow of blood or totally block the flow of blood.
- time dependent
Time dependency occurs when greater therapeutic effects are seen with lower blood levels over a longer period of time.
- transient ischemic attack (TIA)
Occurs when blood flow is interrupted to the brain, even for just a few seconds, resulting in loss of consciousness or temporary loss of neurological function.
- tremor
Usually tremor at rest; When person sits, arm shakes; tremor stops when person attempts to grab something (pill rolling tremor).
- tropic hormones
Hormones that turn on or off the function of other endocrine glands, including ACTH, FSH, LH, and TSH.
- trough
The trough level of medication indicates the lowest concentration of that medication in a person's body. Troughs of medication concentration occur after the drug has been broken down and metabolized by the body.
- type 1 diabetes
An autoimmune disease that affects the beta cells of the pancreas so they do not produce insulin; thus, synthetic insulin must be administered by injection or infusion.
- type 2 diabetes
A condition where the body’s cells become resistant to the effects of insulin. Over time, the beta cells become exhausted and if blood glucose levels cannot be controlled through a healthy diet and exercise, then oral diabetic medication must be implemented and eventually insulin administration may be required.
- vancomycin-resistant S. aureus (VRSA)
An infection caused by Vancomycin-resistant Staphylococcus aureus that is difficult to treat because it exhibits resistance to nearly all available antibiotics.
- veins
Blood vessels that conduct blood toward the heart (except for pulmonary veins that carry deoxygenated blood from the heart to the lungs).
- venous reserve
Volume of blood located in venous networks within the liver, bone marrow, and integument.
- vertigo
A sense of spinning dizziness. It is a symptom of a range of conditions. It can happen when there is a problem with the inner ear, brain, or sensory nerve pathway.
- vestibular system
An area located within the inner ear that gives a sense of balance and spatial orientation for the purpose of coordinating movement with balance.
- vomiting center
An area in the brain that initiates vomiting by inhibiting peristalsis and producing retro peristaltic contractions beginning in the small bowel and ascending into the stomach. It also produces simultaneous contractions in the abdominal muscles and diaphragm that generate high pressures to propel the stomach contents upwards.


 is licensed under CC BY 4.0")










 Medication Safety in Transition of Care by World Health Organization, https://apps.who.int/iris/bitstream/handle/10665/325453/WHO-UHC-SDS-2019.9-eng.pdf?ua=1 page 15, licensed under CC BY-NC-SA 3.0")











" by National Institute of General Medical Sciences Image and Video Gallery is licensed under CC NC-SA 3.0")
























" by M is licensed under CC BY-NC 2.0")


 Inhaler.jpg" by MisterNarwhal is licensed under CC BY-SA 4.0")

.png" by RonEJ at English Wikipedia is licensed under CC0 1.0")












![The vagus nerve (parasympathetic] decreases heart rate. Sympathetic cardiac nerves increases heart rate and force of contraction.](https://opentextbc.ca/accessibilitytoolkit/wp-content/uploads/sites/397/2022/05/image7-1.png ""2032 Automatic Innervation.jpg" by OpenStax College is licensed under CC BY 4.0 Access for free at https://openstax.org/books/anatomy-and-physiology/pages/19-4-cardiac-physiology")
















.JPG" by Intropin is licensed under CC BY 3.0")










. Nausea, vomiting, and hiccups: a review of mechanisms and treatment. Anesthesia progress, 57(4), 150–157. doi:10.2344/0003-3006-57.4.150")






.jpg" by unknown is licensed under CC0")



 is licensed under CC BY 4.0")



" by M is licensed under CC BY-NC 2.0")





/10%3A_Overview_of_the_Nervous_System/10.1%3A_Introduction_to_the_Nervous_System/10.1A%3A_Organization_of_the_Nervous_System")



.png" by William Richard Gowers is licensed under CC0")









.jpg" by Wesalius is licensed under CC BY 4.0")


















. Wong-Baker FACES® Pain Rating Scale. Retrieved [Date] with permission from http://www.WongBakerFACES.org")

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.JPG){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.JPG){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.png){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}