Chapter 6. Non-Parenteral Medication Administration
6.2 Safe Medication Administration
In the Institute of Medicine’s often-cited book To Err Is Human: Building a Safer Health System (Kohn, Corrigan, & Donaldson, 2000), it is estimated that approximately 1.5-million preventable adverse drug events (ADEs) occur annually. The Joint Commission (TJC) defines medication errors as any preventable event that may cause inappropriate medication use or jeopardize patient safety (TJC, 2012).
Medication errors are the number-one error in health care (Centers for Disease Control [CDC], 2013). Safe and accurate medication administration is an important and potentially challenging nursing responsibility. Medication administration requires good decision-making skills and clinical judgment, and the nurse is responsible for ensuring full understanding of medication administration and its implications for patient safety.
Medication errors have a substantial impact on health care in Canada (Butt, 2010). When preparing and administering medication, and assessing patients after receiving medication, always follow agency policy to ensure safe practice. Review Table 6.1 for guidelines for safe medication administration.
Safety Considerations:
|
|||
Principle |
Additional Information |
||
| Be vigilant when preparing medications. | Avoid distractions. Some agencies have a no-interruption zone (NIZ), where health care providers can prepare medications without interruptions. | ||
| Check for allergies. | Always ask patient about allergies, types of reactions, and severity of reactions. | ||
| Use two patient identifiers at all times. Always follow agency policy for patient identification. | Use at least two patient identifiers before administration and compare against the MAR. | ||
| Assessment comes before medication administration. | All medications require an assessment (review of lab values, pain, respiratory assessment, cardiac assessment, etc.) prior to medication administration to ensure the patient is receiving the correct medication for the correct reason. | ||
| Be diligent in all medication calculations. | Errors in medication calculations have contributed to dosage errors, especially when adjusting or titrating dosages. | ||
| Avoid reliance on memory; use checklists and memory aids. | Slips in memory are caused by lack of attention, fatigue, distractions. Mistakes are often referred to as attentional behaviours where lack of training or knowledge is the cause of the error. Slips account for most errors in heath care. If possible, follow a standard list of steps for every patient. | ||
| Communicate with your patient before and after administration. | Provide information to patient about the medication before administering it. Answer questions regarding usage, dose, and special considerations. Give the patient an opportunity to ask questions. Include family members if appropriate. | ||
| Avoid workarounds. | A workaround is a process that bypasses a procedure, policy, or problem in a system. For example, a nurse may “borrow” a medication from another patient while waiting for an order to be filled by the pharmacy. These workarounds fail to follow agency policy to ensure safe medication practices. | ||
| Ensure medication has not expired. | Medication may be inactive if expired. | ||
| Always clarify an order or procedure that is unclear. | Always ask for help whenever you are uncertain or unclear about an order. Consult with the pharmacist, charge nurse, or other health care providers and be sure to resolve all questions before proceeding with medication administration. | ||
| Use available technology to administer medications. | Bar-code scanning (eMAR) has decreased errors in administration by 51%, and computerized physician orders have decreased errors by 81%. Technology has the potential to help decrease errors. Use technology when administering medications but be aware of technology-induced errors. | ||
| Report all near misses, errors, and adverse reactions. | Reporting allows for analysis and identification of potential errors, which can lead to improvements and sharing of information for safer patient care. | ||
| Be alert to error-prone situations and high-alert medications. | High-alert medications are those that are most likely to cause significant harm, even when used as intended. The most common high-alert medications are anticoagulants, narcotics and opiates, insulins, and sedatives. The types of harm most commonly associated with these medications include hypotension, delirium, bleeding, hypoglycemia, bradycardia, and lethargy. | ||
| If a patient questions or expresses concern about a medication, stop and do not administer it. | If a patient questions a medication, stop and explore the patient’s concerns, review the physician’s order, and, if necessary, notify the practitioner in charge of the patient. | ||
| Data source: Agency for Healthcare Research and Quality, 2014; Canadian Patient Safety Institute, 2012; Debono et al., 2013; Institute for Healthcare Improvement, 2015; National Patient Safety Agency, 2009; National Priority Partnership, 2010; Prakash et al., 2014 | |||
Technological Advances That Help Mitigate Medication Errors
Computerized physician order entry (CPOE) is a system that allows prescribers to electronically enter orders for medications, thus eliminating the need for written orders. CPOE increases the accuracy and legibility of medication orders; the potential for the integration of clinical decision support; and the optimization of prescriber, nurse, and pharmacist time (Agrawal, 2009). Decision support software integrated into a CPOE system can allow for the automatic checking of drug allergies, dosage indications, baseline laboratory results, and potential drug interactions. When a prescriber enters an order through CPOE, the information about the order will then transmit to the pharmacy and ultimately to the MAR.
The use of electronic bar codes on medication labels and packaging has the potential to improve patient safety in a number of ways. A patient’s MAR is entered into the hospital’s information system and encoded into the patient’s wristband, which is accessible to the nurse through a handheld device. When administering a medication, the nurse scans the patient’s medical record number on the wristband, and the bar code on the drug. The computer processes the scanned information, charts it, and updates the patient’s MAR record appropriately (Poon et al., 2010).
Automated medication dispensing systems (AMDS) provide electronic automated control of all medications, including narcotics. Each nurse accessing the system has a unique access code. The nurse will enter the patient’s name, the medication, the dosage, and the route of administration. The system will then open either the patient’s individual drawer or the narcotic drawer to dispense the specific medication. If the patient’s electronic health record is linked to the AMDS, the medication and the nurse who accessed the system will be linked to the patient’s electronic record.
Checklist 43 outlines the steps for safe medication administration.
Disclaimer: Always review and follow your hospital policy regarding this specific skill. |
|||
Safety considerations:
|
|||
Steps |
Additional Information |
||
| 1. Check MAR against doctor’s orders. | Check that MAR and doctor’s orders are consistent.
 Compare MAR with patient wristband. Night staff usually complete and verify this check as well. |
||
2. Perform the SEVEN RIGHTS x 3 (this must be done with each individual medication):
Medication calculation: D/H x S = A (D or desired dosage/H or have available x S or stock = A or amount prepared) |
The right patient: check that you have the correct patient using two patient identifiers (e.g., name and date of birth).
 The right medication (drug): check that you have the correct medication and that it is appropriate for the patient in the current context. The right dose: check that the dose makes sense for the age, size, and condition of the patient. Different dosages may be indicated for different conditions. The right route: check that the route is appropriate for the patient’s current condition. The right time: adhere to the prescribed dose and schedule.  The right reason: check that the patient is receiving the medication for the appropriate reason. The right documentation: always verify any unclear or inaccurate documentation prior to administering medications. NEVER document that you have given a medication until you have actually administered it. |
||
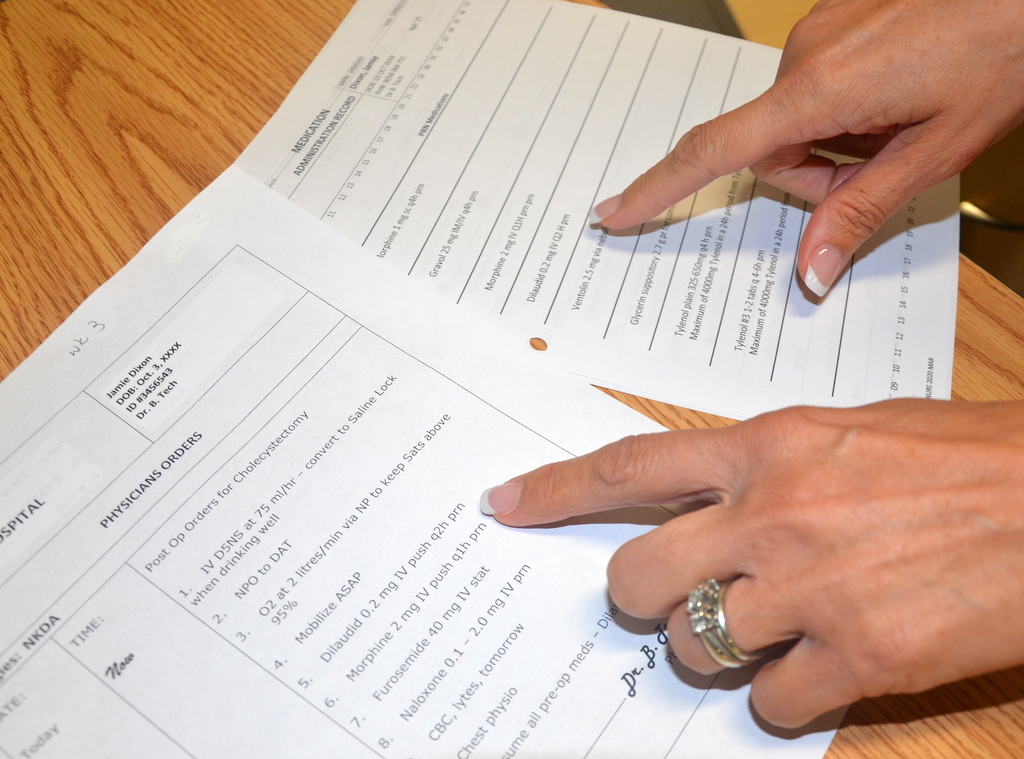
3. The label on the medication must be checked for name, dose, and route, and compared with the MAR at three different times:
|
 These checks are done before administering the medication to your patient. If taking the drug to the bedside (e.g., eye drops), do a third check at the bedside. |
||
| 4. Circle medication when poured. | Pour medication. Circle MAR to show that medication has been poured.
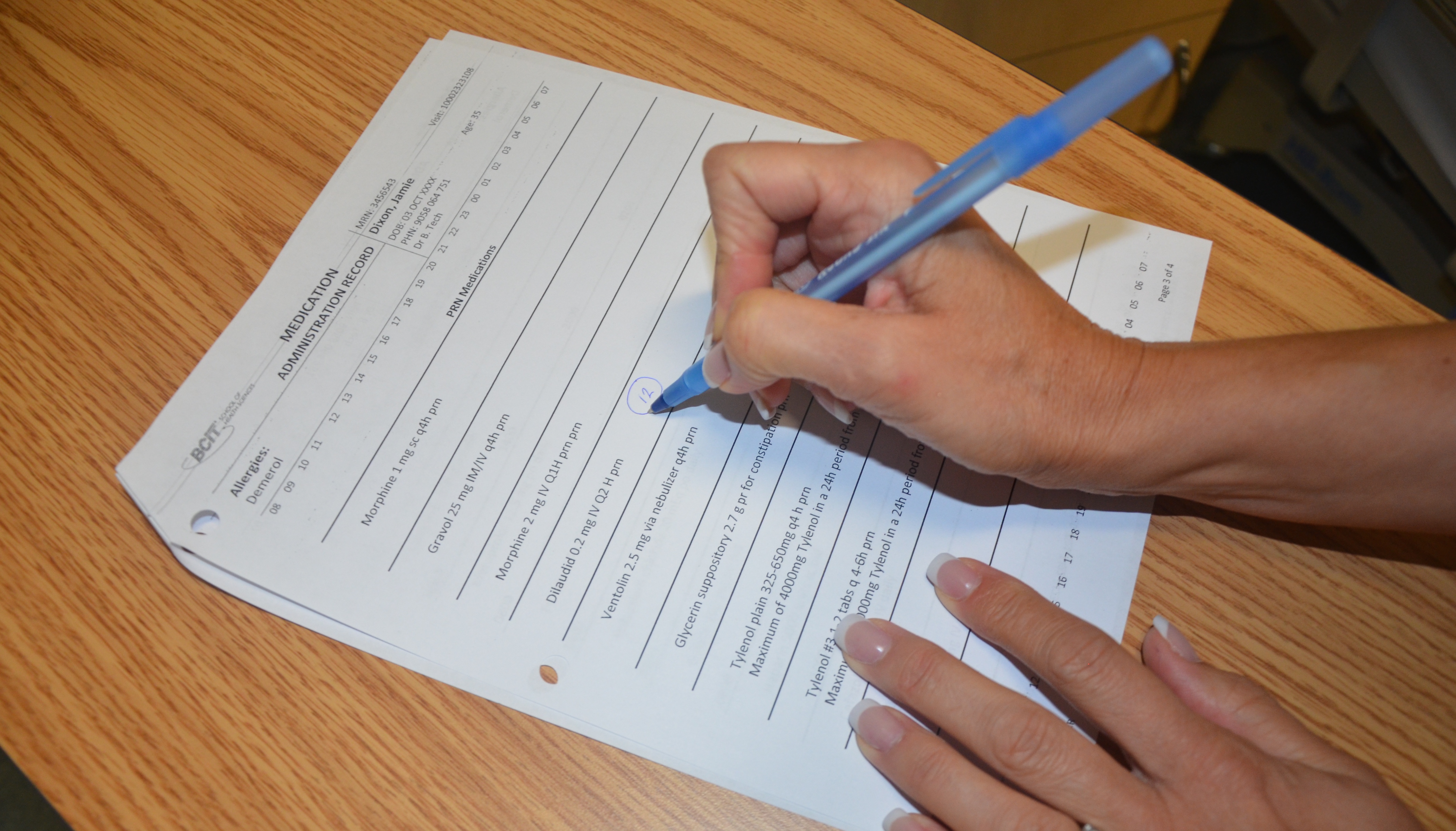 |
||
5. Positioning:
|
This ensures patient safety and comfort.
 |
||
6. Post-medication safety check:
|
This ensures patient safety.
This step prevents the transfer of microorganisms.  |
||
| Data source: Lilley, Harrington, Snyder, & Swart, 2011; Lynn, 2011; Perry et al., 2014 | |||
Critical Thinking Exercises
- Discuss why you think medication reconciliation is important for patient safety.
- List five steps you can take to ensure safe medication administration practice.
