Chapter 10. Tubes and Attachments
10.3 Nasogastric Tubes
Using a Nasogastric Tube
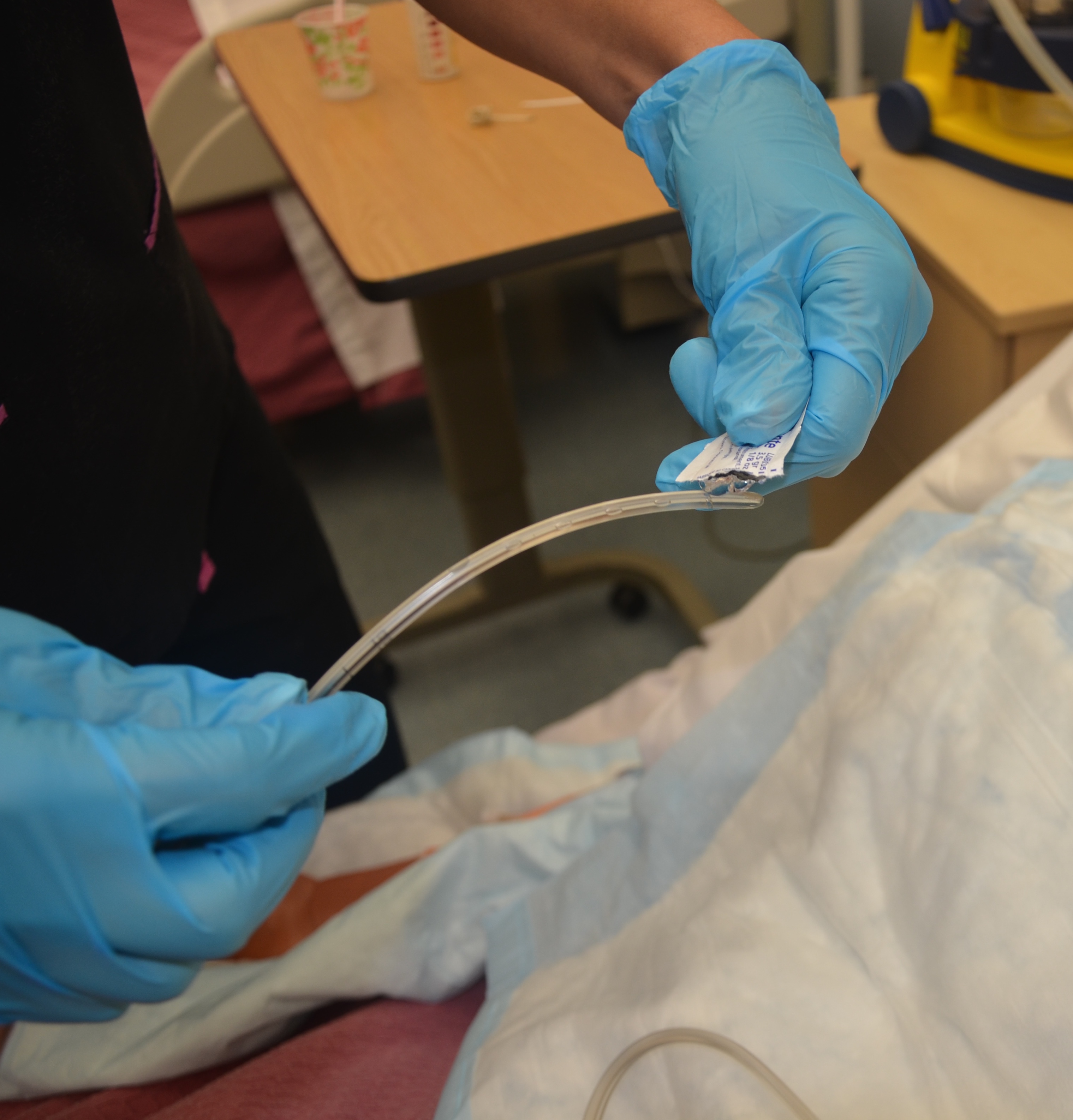
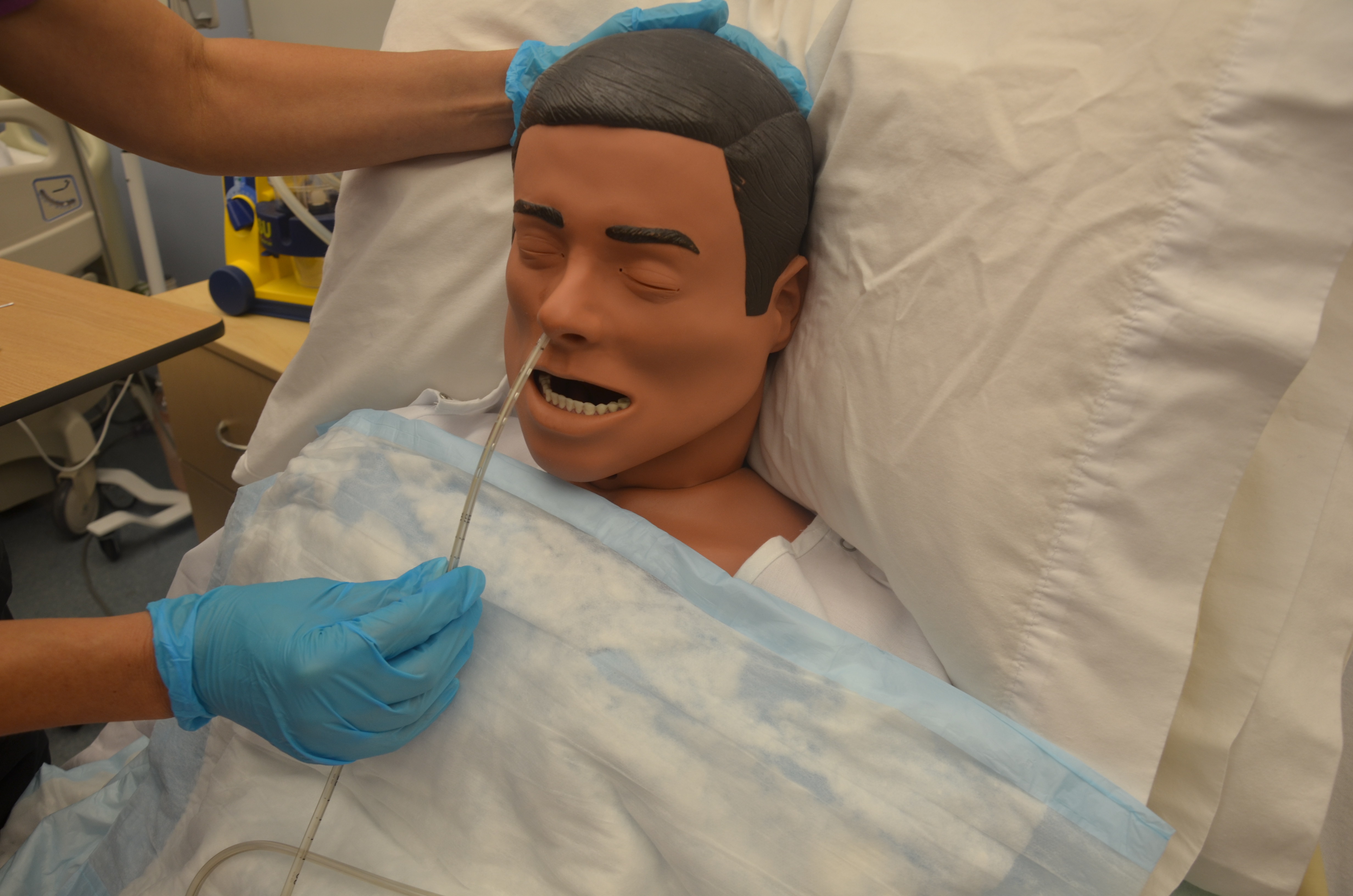
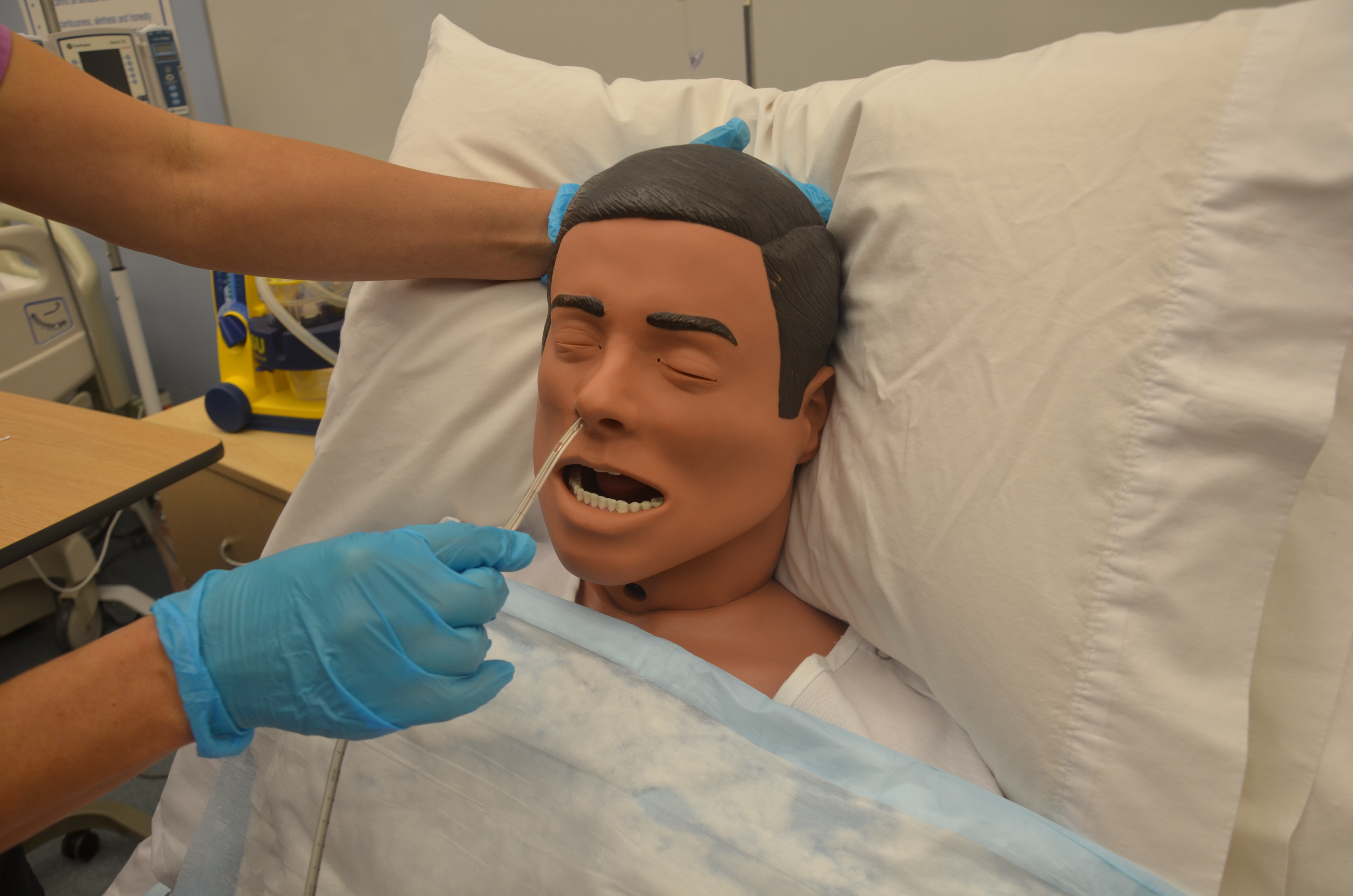
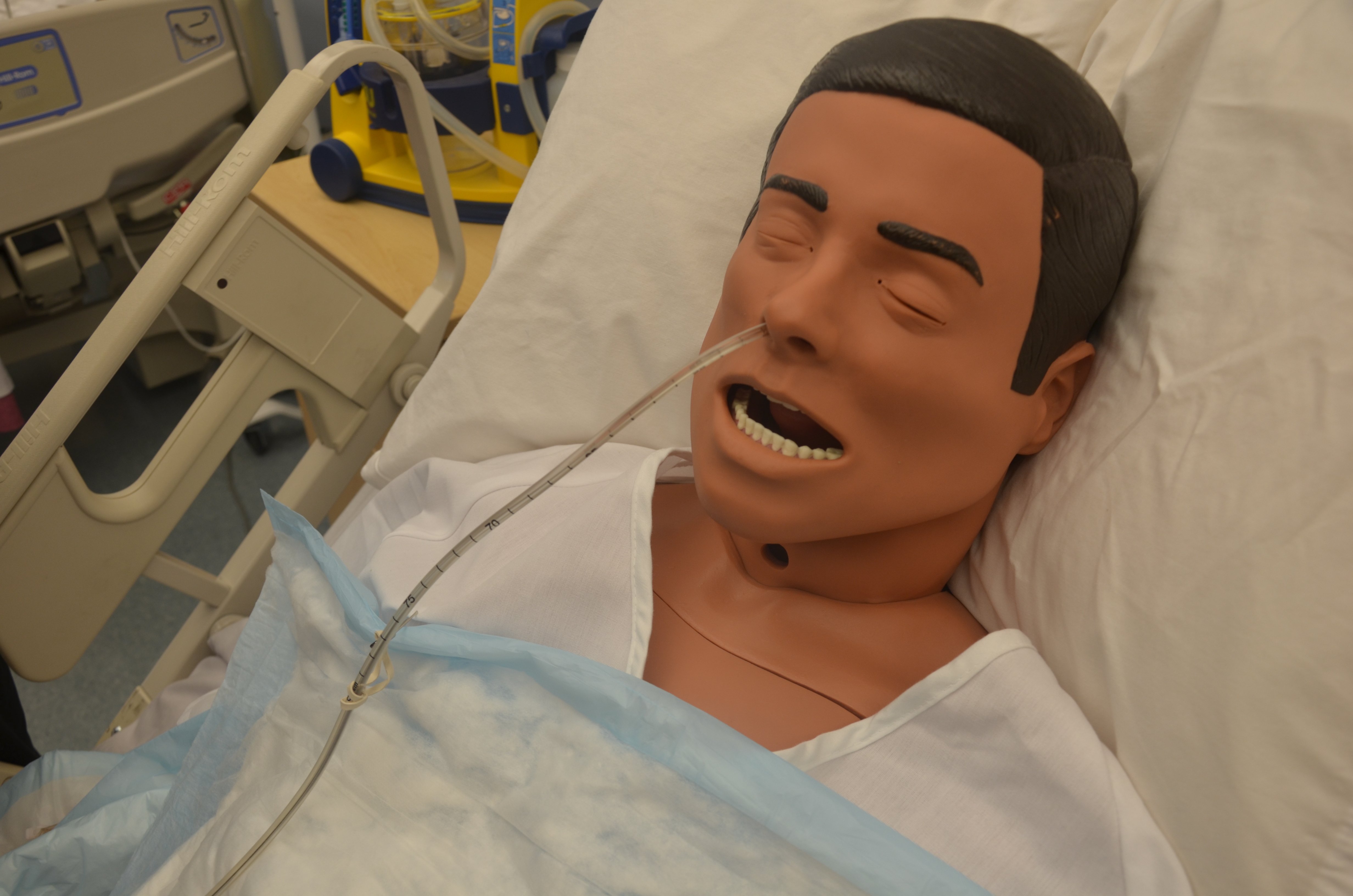
A nasogastric (NG) tube is a flexible plastic tube inserted through the nostrils, down the nasopharynx, and into the stomach or the upper portion of the small intestine. Placement of NG tubes is always confirmed with an X-ray prior to use (Perry, Potter, & Ostendorf, 2014).
NG tubes are used to:
- Deliver nutrients to the patient via a feeding pump
- Remove gastric contents
An NG tube used for feeding should be labelled. The tube is used to feed patients who may have swallowing difficulties or require additional nutritional supplements. These tubes are narrower and smaller bored than a Salem sump or Levine tube.
An NG tube can also remove gastric content, either draining the stomach by gravity or by being connected to a suction pump. In these situations, the NG tube is used to prevent nausea, vomiting, or gastric distension, or to wash the stomach of toxins.
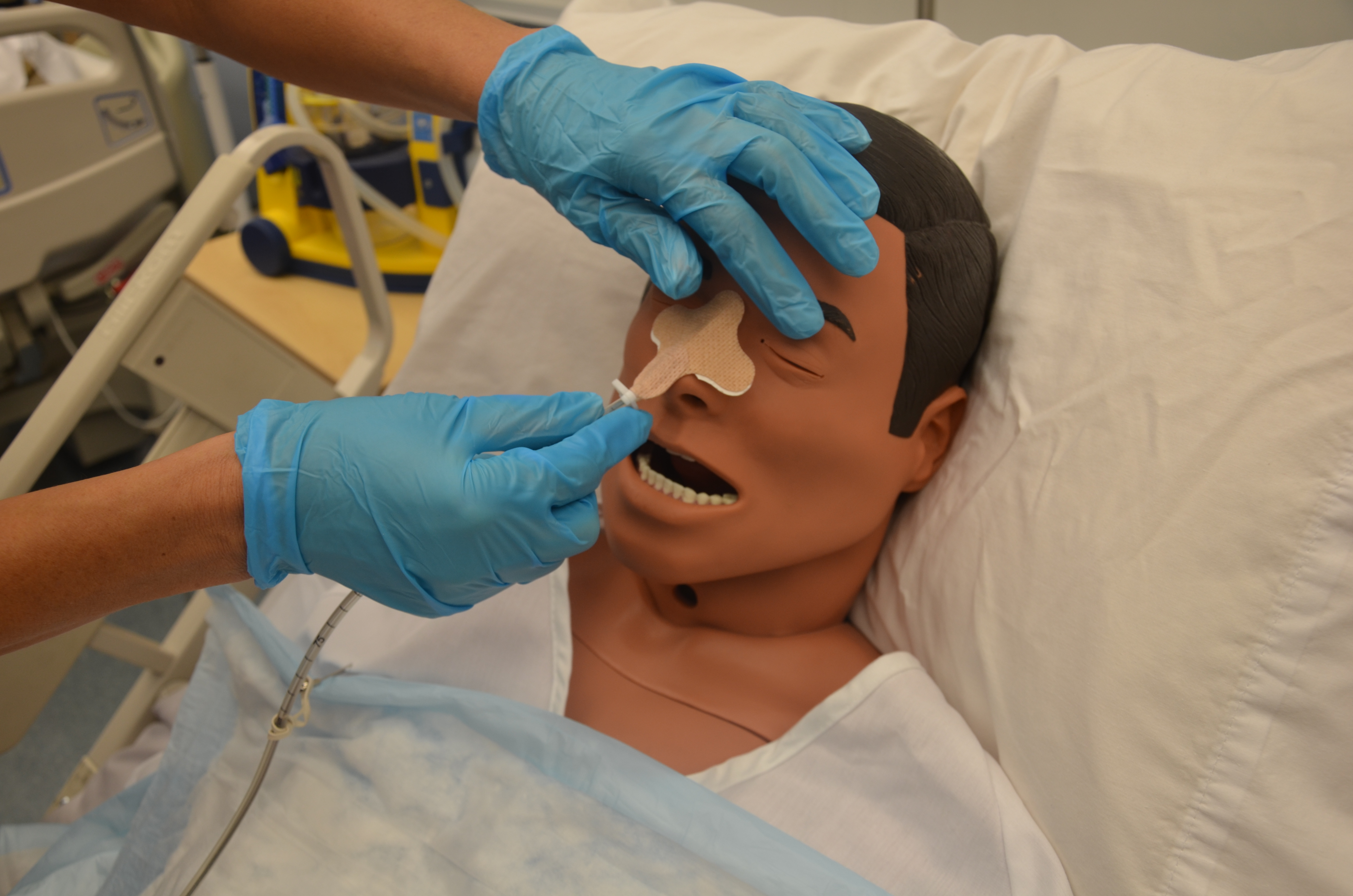
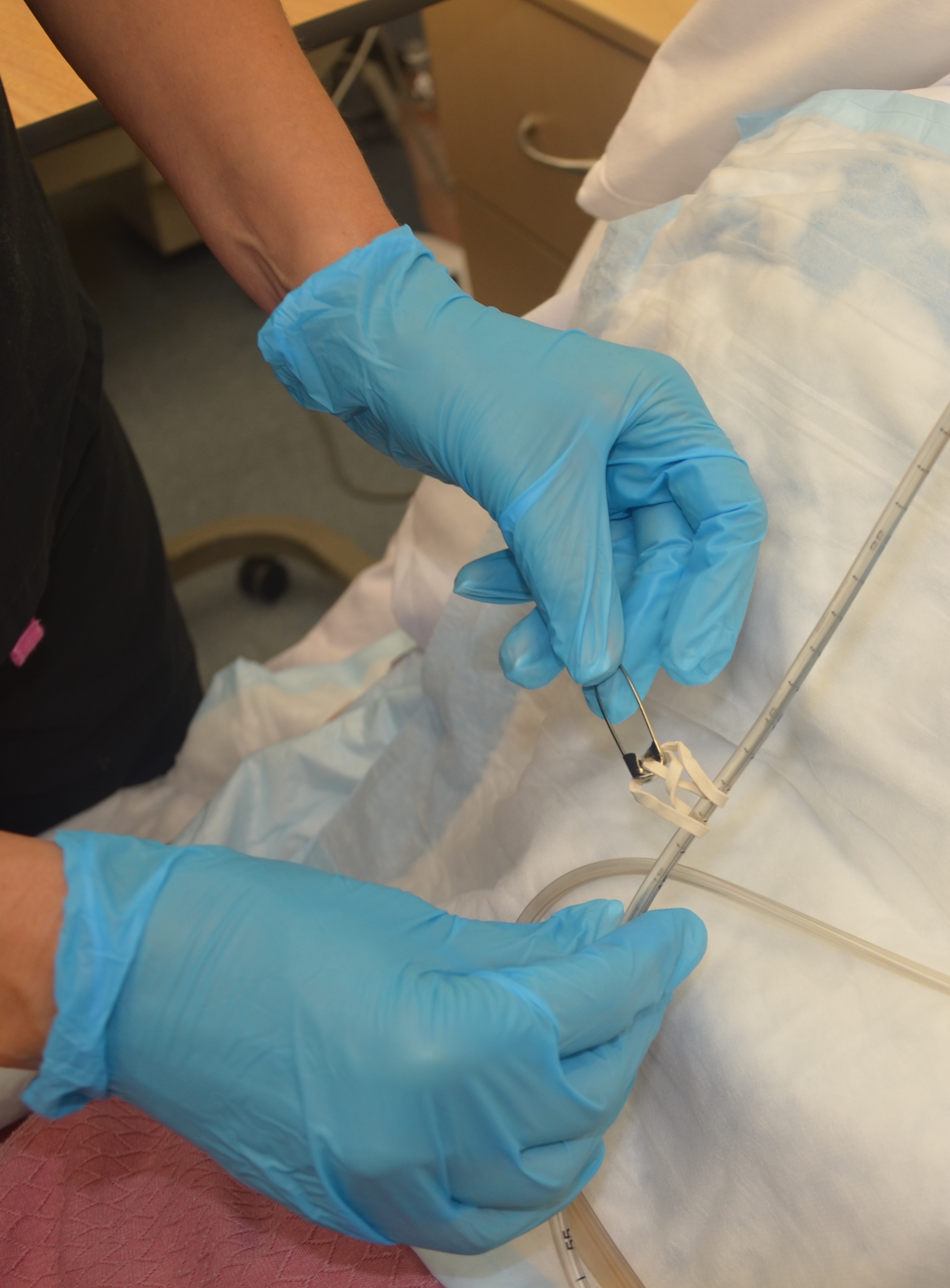
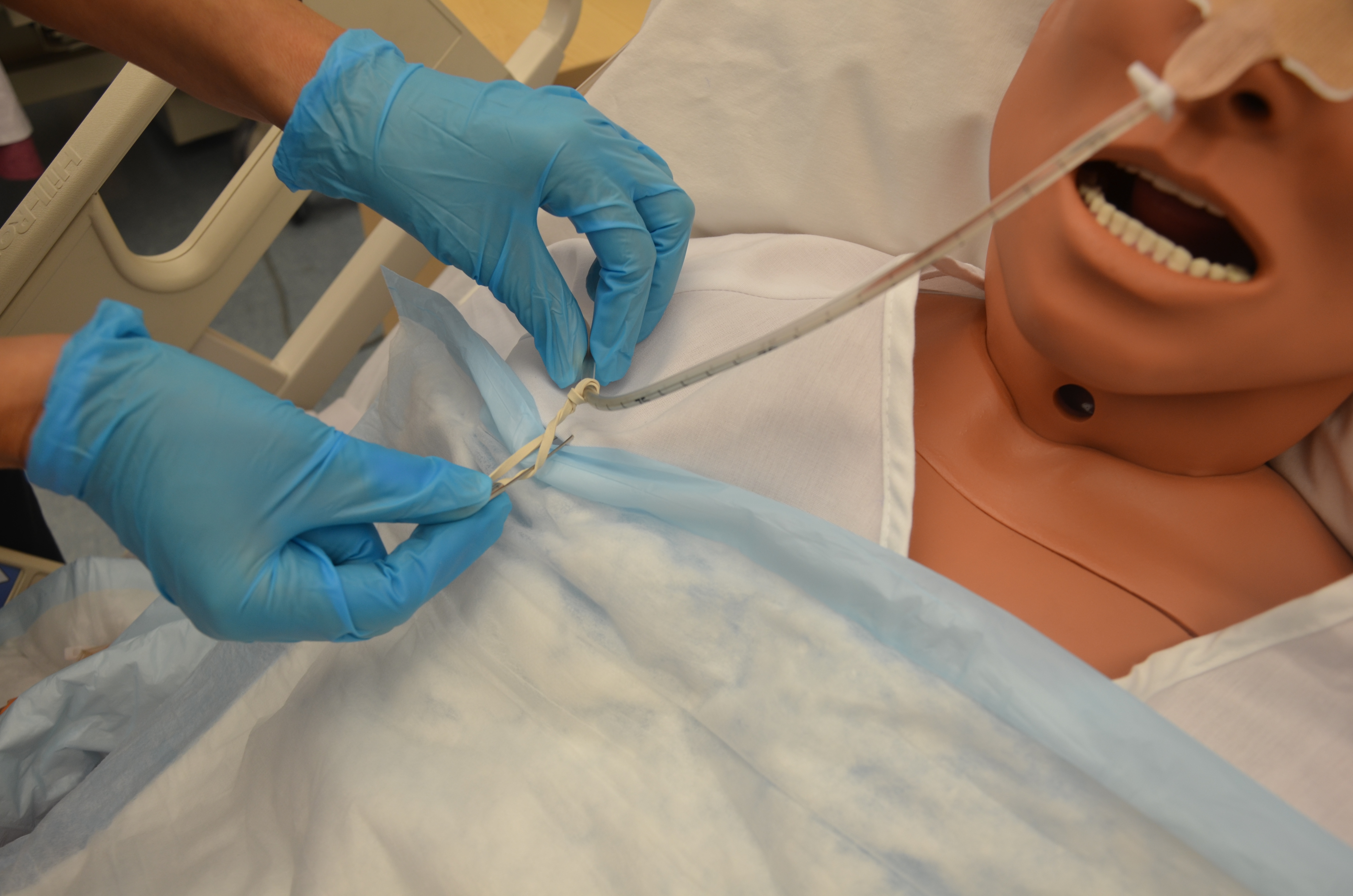
The NG tube is fastened to the patient using a nose clip, and is taped and pinned to the patient’s gown to prevent accidental removal of the tube and to prevent the tube from slipping from the stomach area into the lungs.
When working with people who have nasogastric tubes, remember the following care measures:
- Maintain and promote comfort. The tube constantly irritates the nasal mucosa, causing a great deal of discomfort. Ensure that the tube is securely anchored to the patient’s nose to prevent excess tube movement, and is pinned to the gown to avoid excessive pulling or dragging.
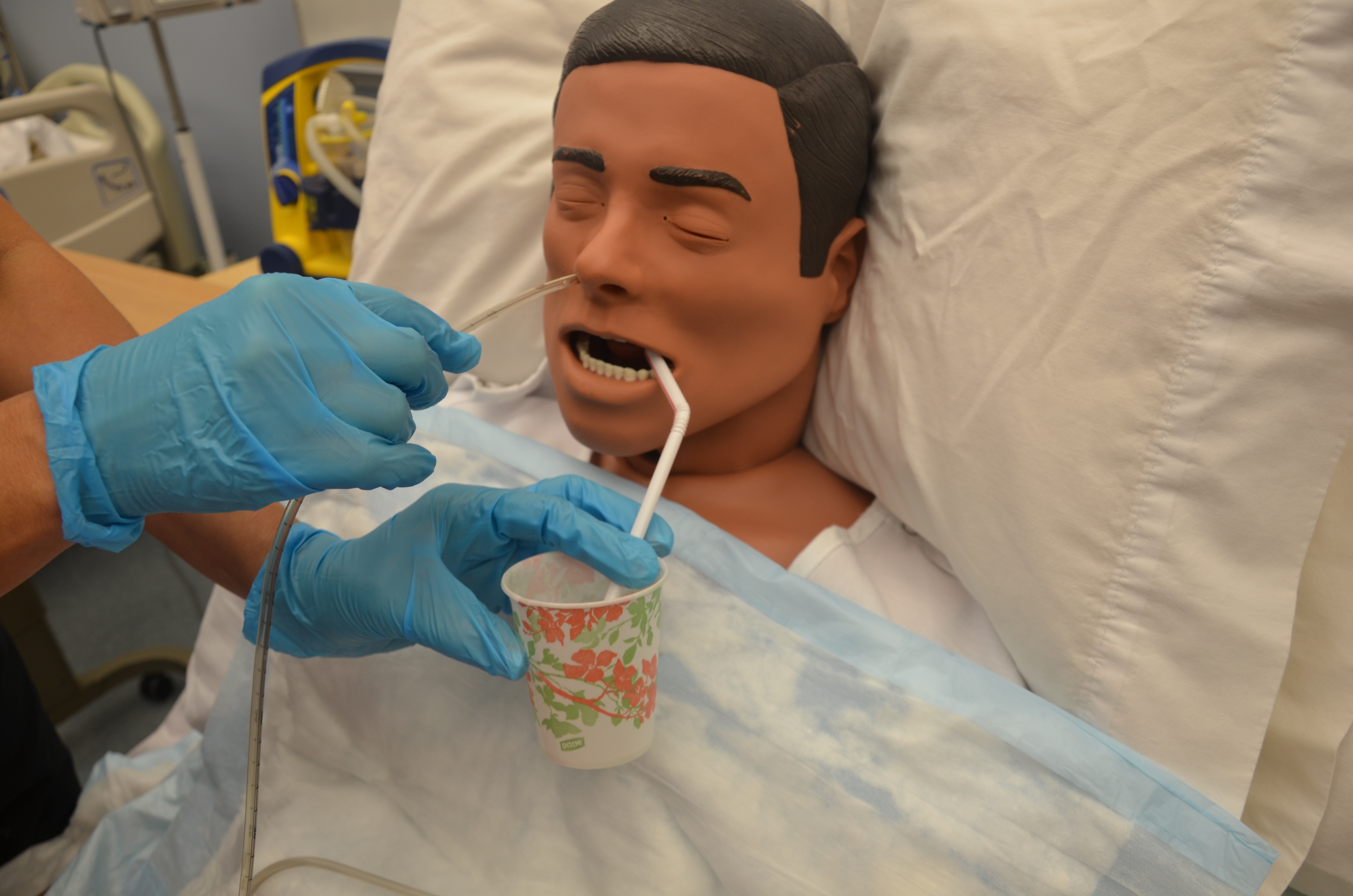
- Because one nostril is blocked, patients tend to mouth breathe. This causes dehydration of the nasal and oral mucosa, and patients will complain of thirst, but they are usually NPO (nil per os or nothing by mouth). Mouth care will help to relieve the dryness. This can include rinsing the mouth with cold water or mouthwash as long as the patient does not swallow. Some patients may be allowed to suck on ice chips.
- If the patient complains of abdominal pain, discomfort, or nausea, or begins to vomit, report it immediately. The drainage flow is probably obstructed and the tube will need to be irrigated.
- These patients should never be allowed to lie completely flat. Lying flat increases the patient’s risk of aspirating stomach contents. Patients with an NG tube are at risk for aspiration. The head of bed should always be raised 30 degrees or higher.
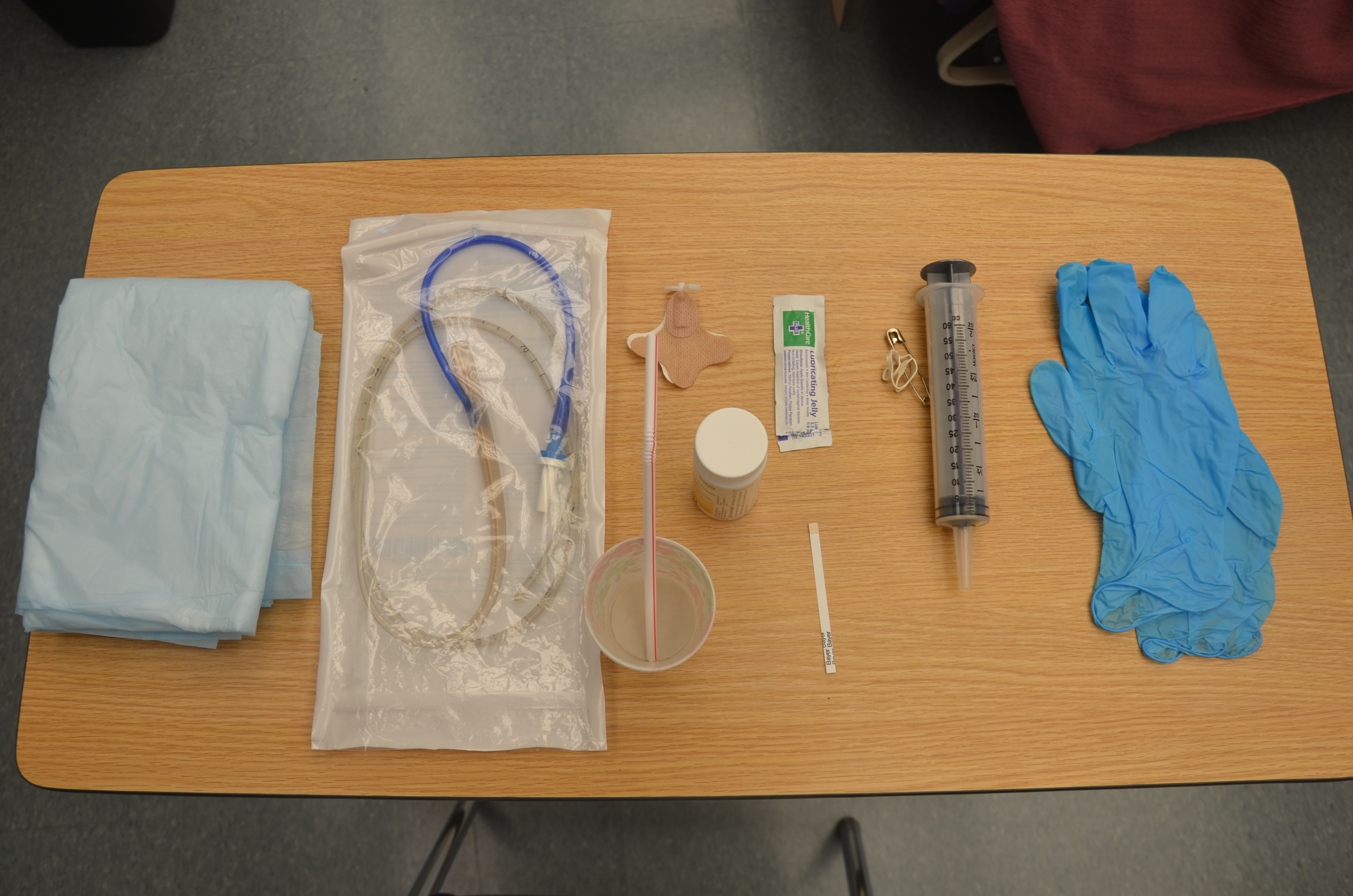
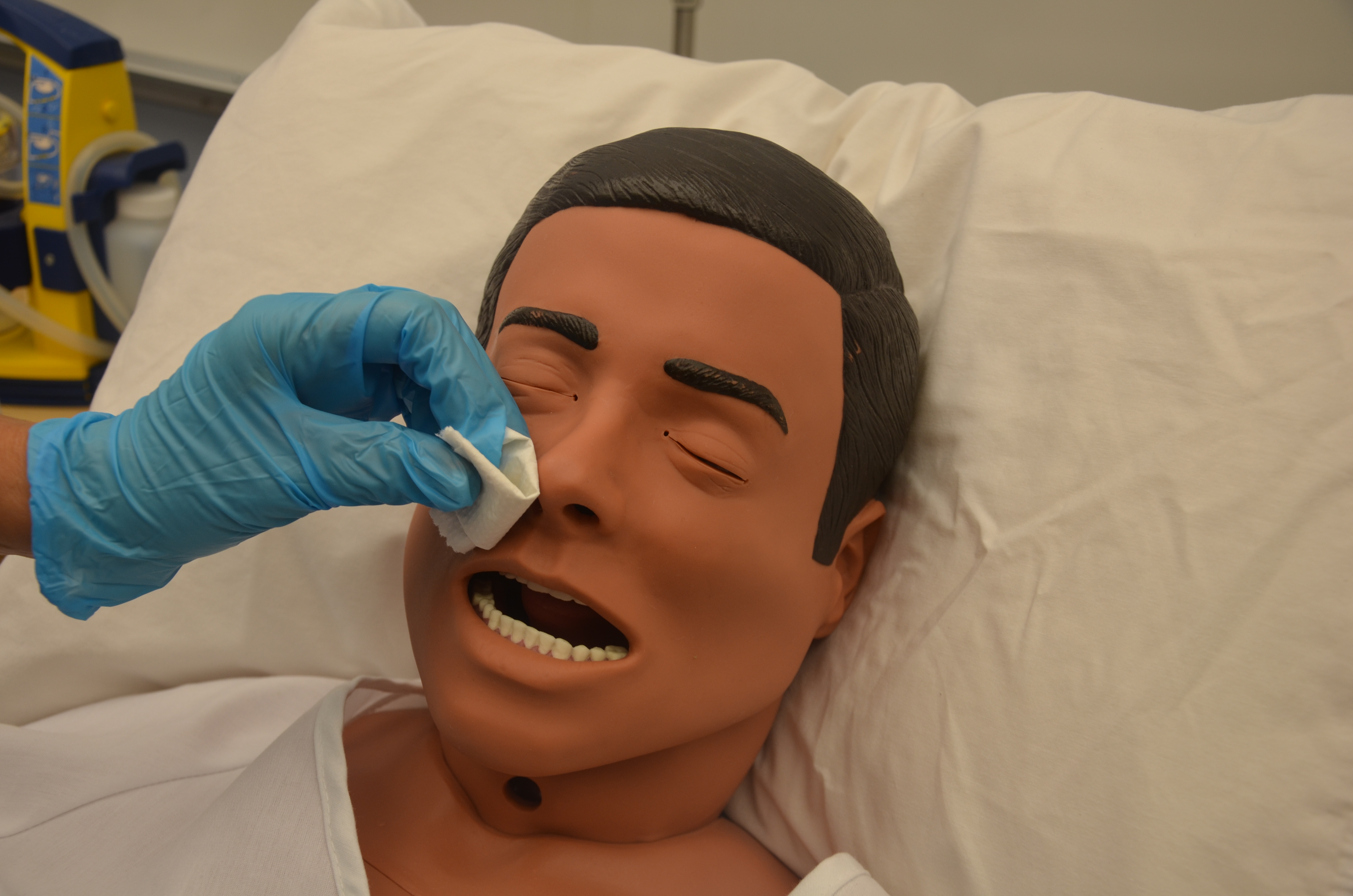
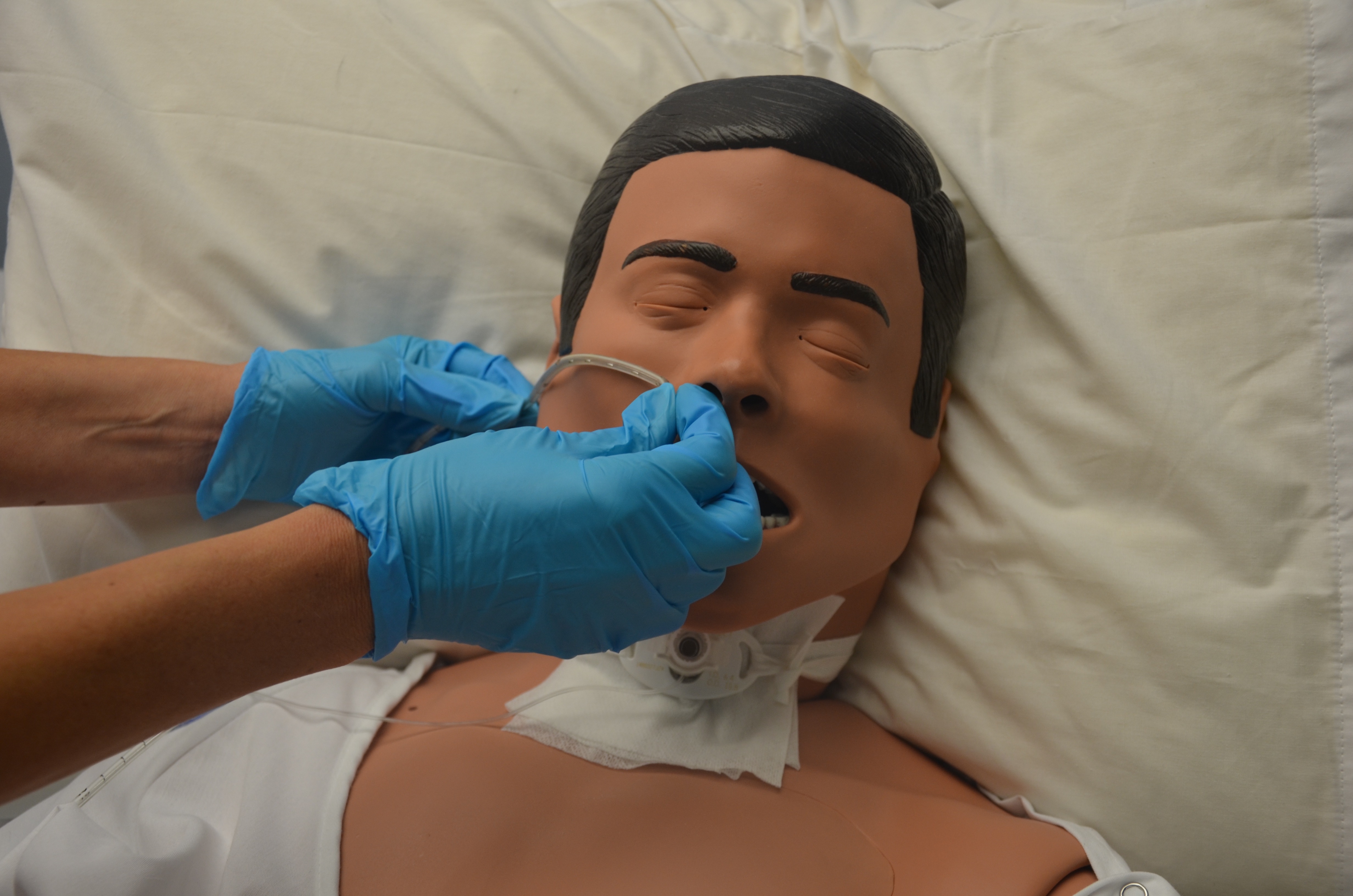
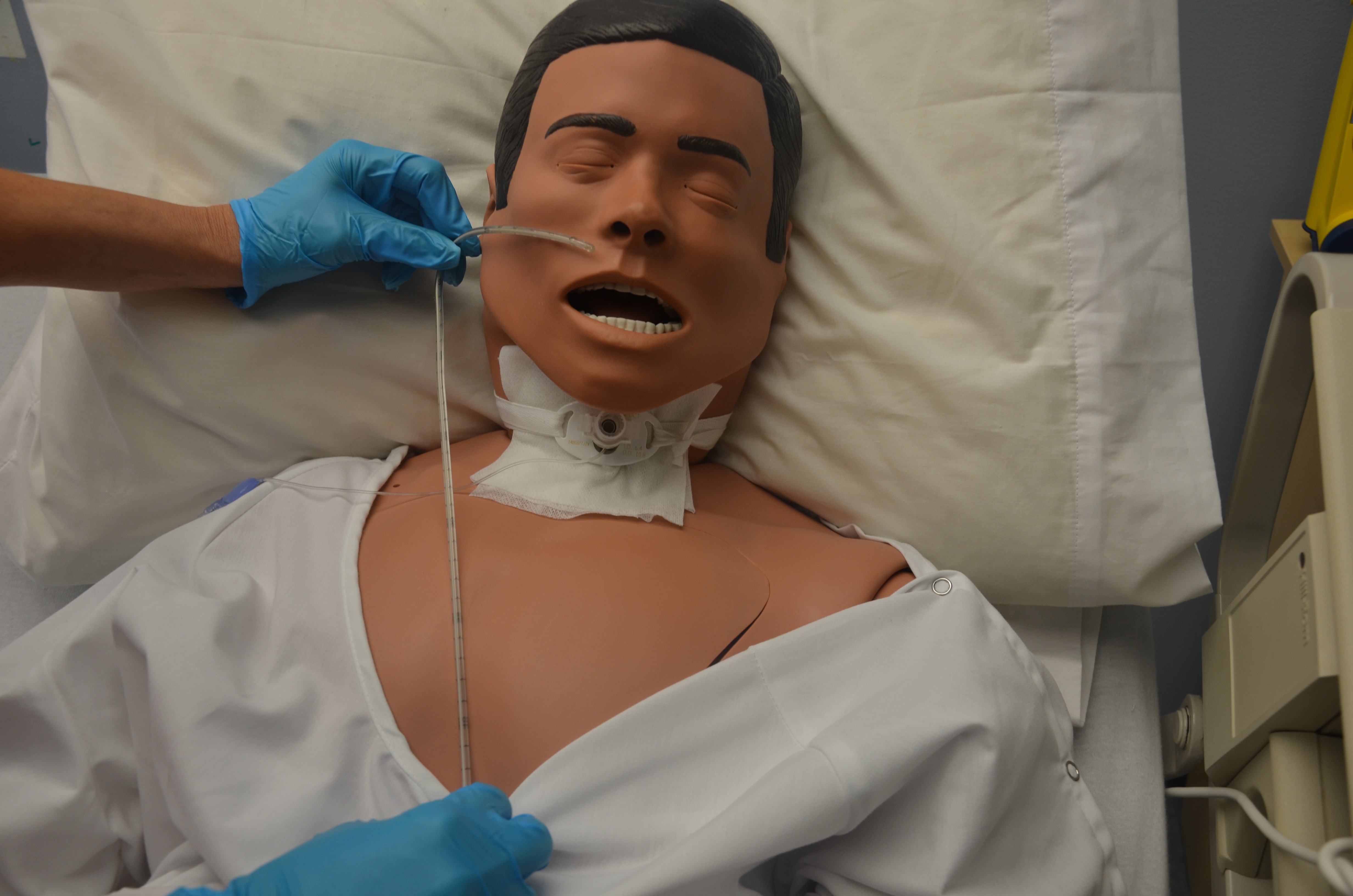
Checklist 78 outlines the steps for inserting a nasogastric tube.

Special considerations with NG tubes:
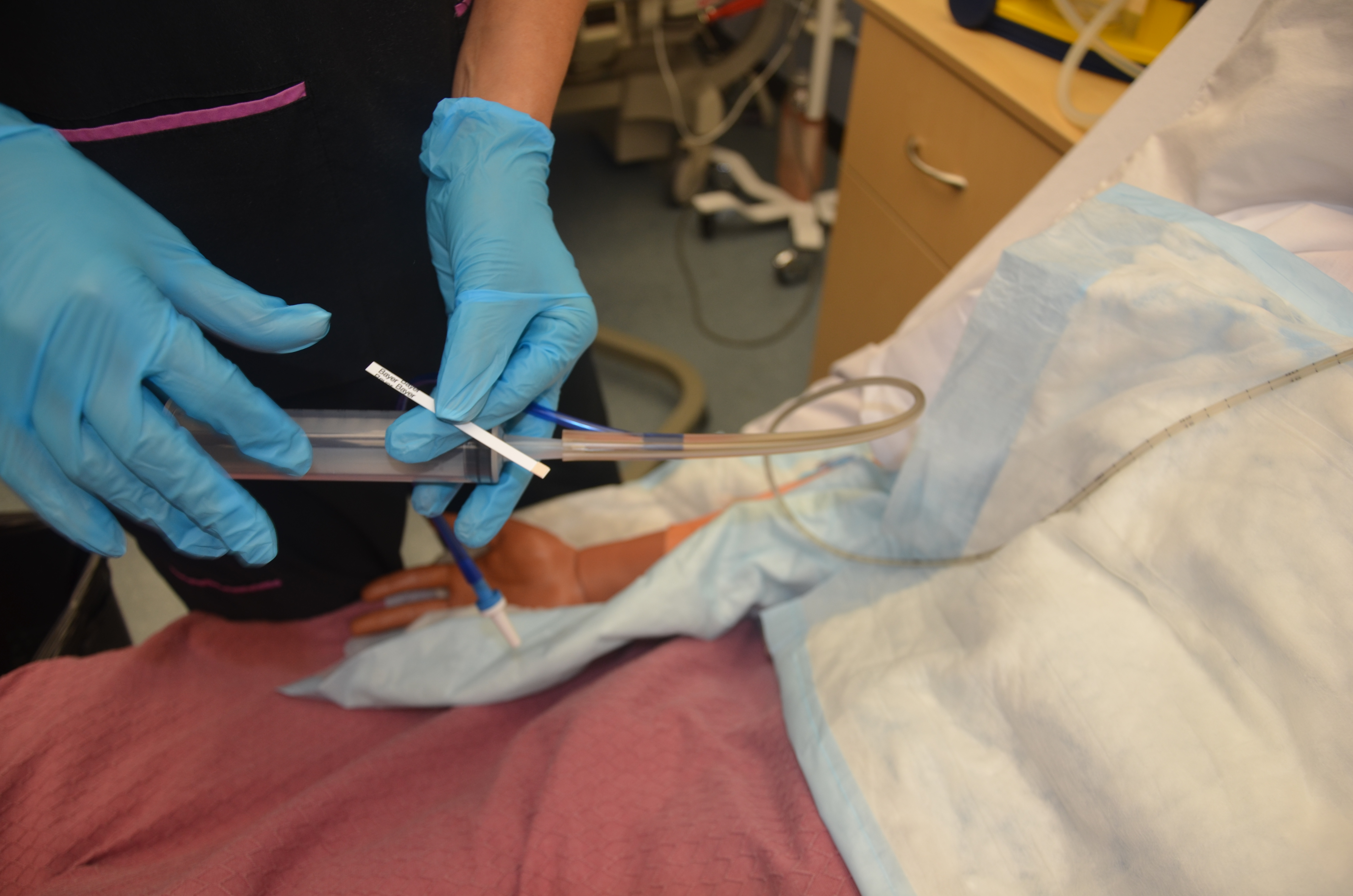
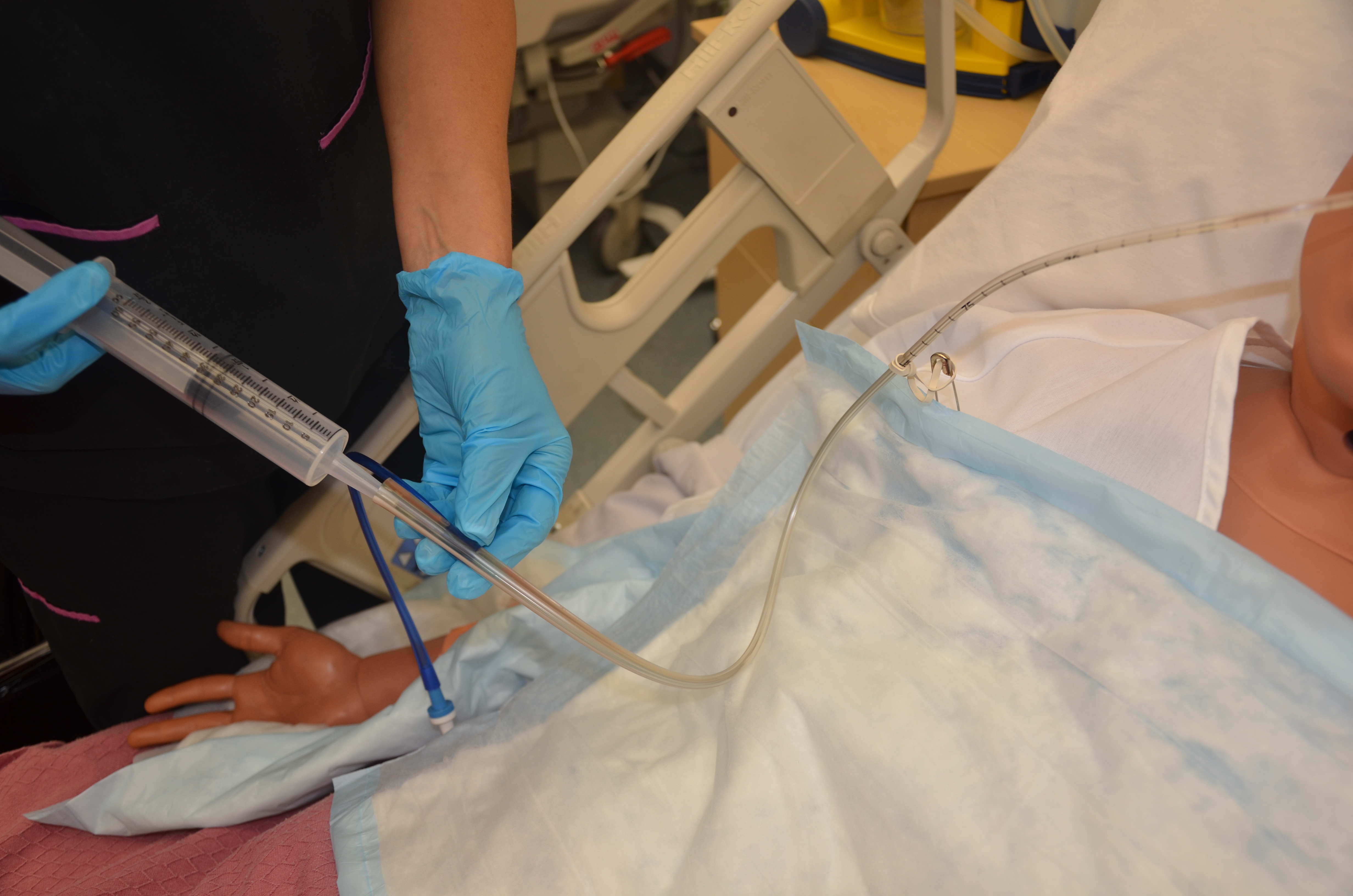
- Always assess correct placement of the NG tube prior to infusing any fluids or tube feeds as per agency policy. Check location of external markings on the tube and colour of the PH of fluid aspirated from the tube. Routine evaluation will ensure the correct placement of the tube and reduce the risk of aspiration. Do not instill air to test location of tube.
- Do not give the patient anything to eat or drink without knowing that the patient has passed a swallowing assessment.
- If changing the gown or repositioning the patient, take care not to pull on the NG tube. Remember to unpin the tube from the gown and repin the tube.
- If the NG tube falls out of the patient, it is not an emergency. But be sure to assess your patient. How are the ABCCS? Notify the RN in charge of the patient.
- A patient who appears to be in respiratory distress should be considered an emergency, and emergency procedures should be followed. Respiratory distress may present as coughing, choking, or reduced oxygen saturation.
Video 10.1
Removing an NG Tube
An NG tube should be removed if it is no longer required. The process of removal is usually very quick. Prior to removing an NG tube, verify physician orders. If the NG tube was ordered to remove gastric content, the physician’s order may state to “trial” clamping the tube for a number of hours to see if the patient tolerates its removal. During the trial, the patient should not experience any nausea, vomiting, or abdominal distension.
To review how to remove an NG tube, refer to Checklist 79.





Critical Thinking Exercises
- You are inserting a nasogastric tube and the tube is not advancing. Explain your next steps, with rationale.
- Your patient has a nasogastric tube and is requesting water because her throat feels dry. Describe your next actions.
