Chapter 5. Oxygen Therapy
5.6 Management of Hypoxia
Hypoxemia or hypoxia is a medical emergency and should be treated promptly. Failure to initiate oxygen therapy can result in serious harm to the patient. The essence of oxygen therapy is to provide oxygen according to target saturation rate, and to monitor the saturation rate to keep it within target range. The target range (SaO2) for a normal adult is 92 – 98%. For patients with COPD, the target SaO2 range is 88 – 92% (Alberta Health Services, 2015; Kane, et al., 2013; Perry et al., 2014).
Although all medications require a prescription, oxygen therapy may be initiated without a physician’s order in emergency situations. Hypoxia is considered an emergency situation. Most hospitals have a protocol in place allowing health care providers to apply oxygen in emergency situations. The health care provider administering oxygen is responsible for monitoring the patient response and keeping the oxygen saturation levels within the target range. The most common reasons for initiating oxygen therapy include acute hypoxemia related to pneumonia, shock, asthma, heart failure, pulmonary embolus, myocardial infarction resulting in hypoxemia, post operative states, pneumonthorax, and abnormalities in the quality and quantity of hemoglobin. There are no contradictions to oxygen therapy if indications for therapy are present (Kane et al., 2013).
Hypoxic patients must be assessed for the causes and underlying reasons for their hypoxia. Hypoxia must be managed not only with supplemental oxygen but in conjunction with the interventions outlined in Table 5.3.
| Interventions |
Additional Information |
||
| Raise the head of the bed | Raising the head of the bed promotes effective breathing and diaphragmatic descent, maximizes inhalation, and decreases the work of breathing. Positioning enhances airway patency in all patients. A Fowler’s or semi-Fowler’s position promotes a patient’s chest expansion with the least amount of effort. Patients with COPD who are short of breath may gain relief by sitting with their back against a chair and rolling their head and shoulders forward or leaning over a bedside table while in bed.
 |
||
| Deep breathing and coughing techniques | Deep breathing and coughing techniques help patients effectively clear their airway while maintaining their oxygen levels. Teach patients “controlled coughing” by having them take a deep breath in and cough deeply with the mouth slightly open. If they have difficulty coughing, teach the huffing technique. This involves taking a medium breath and then making a sound like “ha” to push the air out fast with the mouth slightly open. This is done three or four times, and then they are instructed to cough. If secretions are thick and tenacious, the patient may be dehydrated and require additional fluids (if medical condition does not contraindicate additional fluids). | ||
| Oxygen therapy and equipment | If patient is already on supplemental oxygen, ensure equipment is turned on and set at the required flow rate and is connected to an oxygen supply source. If a portable tank is being used, check the oxygen level in the tank. Ensure the connecting oxygen tubing is not kinked, which could obstruct the flow of oxygen. Feel for the flow of oxygen from the exit ports on the oxygen equipment. In hospitals where medical air and oxygen are used, ensure patient is connected to the oxygen flow port.
 |
||
| Assess need for bronchodilators | Pharmacological management is essential for patients with respiratory disease. Medications such as bronchodilators effectively relax smooth muscles and open airways in certain disease processes such as COPD. Glucocorticoids relieve inflammation and also assist in opening air passages. Mucolytics and adequate hydration decrease the thickness of pulmonary secretions so that they can be expectorated more easily.
 |
||
| Oral suctioning | Some patients may have a weakened cough that inhibits their ability to clear secretions from the mouth and throat. Patients with muscle disorders or who have experienced a cerebral vascular accident (CVA) are at risk for aspiration related to ineffective cough reflex, which could lead to hypoxia. Provide oral suction if patient is unable to clear secretions, foreign debris, or mucous from the mouth and pharynx. See Checklist 42 for further directions.
 |
||
| Pain relief | Provide adequate pain relief. Pain is known to increase the metabolic demands on the body, which in turn increases the need for more oxygen supply. | ||
| Devices to enhance secretion clearance | Many devices assist with secretion clearance, such as vests that inflate with large volumes of air and vibrate the chest wall, and handheld devices that help provide positive expiratory pressure to prevent airway collapse in exhalation. Usefulness of these therapies is decided based on the individual patient’s situation and the preference of both the patient and care provider. | ||
| Frequent rests in between activities | Patients experiencing hypoxia often feel short of breath (SOB) and fatigue easily. Allow patient to rest frequently, and space out interventions to decrease oxygen demand in patients whose reserves are likely limited. Has the patient just returned from a walk down the hall or to the bathroom?
Assess for underlying causes of the hypoxia. Is the potential problem respiratory or cardiovascular? What underlying respiratory or cardiovascular conditions exist? Complete respiratory and cardiovascular assessments may reveal potential abnormalities in these systems. |
||
| Obstructive sleep apnea | Patients with obstructive sleep apnea (OSA) may be unable to maintain a patent airway. In OSA, nasopharyngeal abnormalities that cause narrowing of the upper airway produce repetitive airway obstruction during sleep, with the potential for periods of apnea and hypoxemia. Pressure can be delivered during the inspiratory and expiratory phases of the respiratory cycle by using a mask to maintain airway patency during sleep. The process requires consideration of each individual’s needs in order to to obtain compliance. | ||
| Anxiety and depression | The most common co-morbidities of COPD are anxiety and depression. Anxiety is related to chronic shortness of breath and an inability to breathe effectively. Anxiety and depression are chronically undertreated and may be relieved with breathing retraining, counselling, relaxation techniques, or anti-anxiety medications if appropriate. | ||
| Data source: Cigna & Turner-Cigna, 2005; Kane et al., 2013; Maurer et al., 2008; Perry et al., 2007; Perry et al., 2014; Shackell & Gillespie, 2009 | |||
Applying and Titrating Oxygen Therapy
When providing oxygen therapy, remember the following (Kane et al., 2013):
- Initiate oxygen according to hospital protocols when patients with respiratory or cardiovascular conditions warrant its use.
- Always assess for underlying respiratory diseases. Patients with COPD are at risk for acute hypoventilation and carbon dioxide retention. Elevated CO2 levels increase risk for respiratory failure or hyperventilation. With COPD patients, always check the physician orders for the required amount of oxygen and acceptable SaO2 range.
- Regardless of underlying conditions, your first priority should be to prevent or treat hypoxia. Never withhold oxygen for COPD patients while waiting for additional medical interventions (Alberta Health Services, 2015; British Thoracic Society, 2008).
- Check all equipment for safety and function at least once per shift. Check oxygen equipment more frequently if using a high-flow system, which requires higher oxygen concentration.
- Avoid interruption of oxygen therapy during patient transport.
- When patient has a tracheostomy or a high-flow oxygen system and is being transported out of your care, contact respiratory therapy for assistance.
Oxygen is available in hospitals through bulk liquid oxygen systems that dispense oxygen as a gas through outlets in rooms. It can also be provided in cylinders (large or small) for easy transport for patient use while mobile or when moving around the hospital. An oxygen flow meter regulates the flow in litres per minute. Oxygen therapy may be short- or long-term depending on the SaO2 requirements of the patients and underlying diseases processes (Perry et al., 2014).
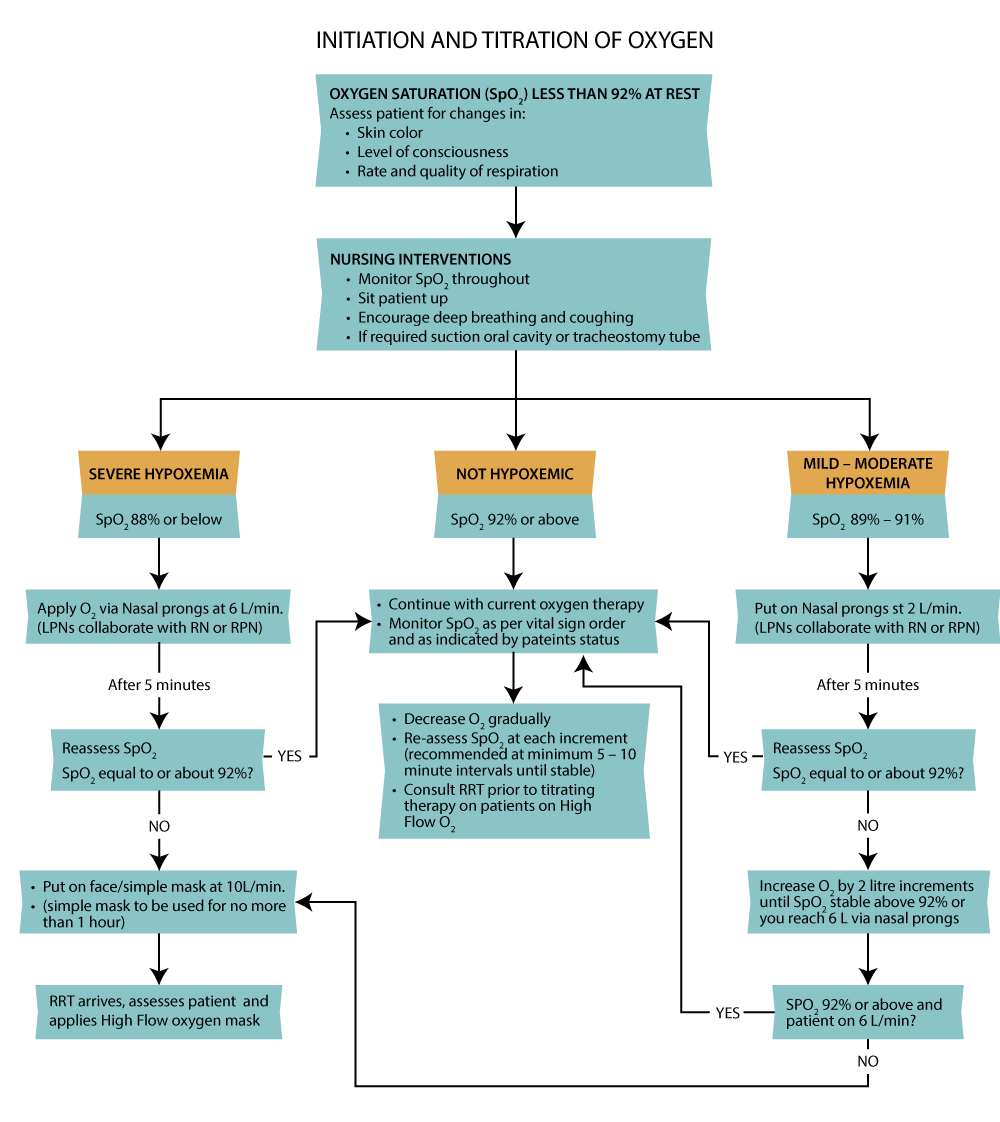
Checklist 41 reviews the steps for applying and titrating oxygen therapy (see Figure 5.2).
Disclaimer: Always review and follow your hospital policy regarding this specific skill. |
|||
Safety considerations:
|
|||
Steps |
Additional Information |
||
| 1. Complete respiratory assessment for hypoxia. SaO2 should be greater than 92% unless otherwise stated by the physician. The goal is to use the least amount of oxygen to maintain levels between 92% and 98%. | Assess need for O2: check SaO2 level with a pulse oximetry device.
Assess for underlying medical conditions or alternate causes of hypoxia (cardiovascular). |
||
| 2. If a patient requires oxygen therapy, choose an oxygen delivery system based on your patient’s requirements. | Oxygen is initially started at a low concentration (2 L/min) using nasal prongs. Then the flow is titrated up to maintain oxygen saturation of 92% or greater.
Selection of delivery system is based on the level of oxygen support required (controlled or non-controlled), the severity of hypoxia, and the disease process. Other factors include age, presence of underlying disease (COPD), level of health, presence of an artificial airway, and environment (home or hospital). Significant decreases to O2 saturation levels or large increases to maintain O2 saturation should be reported promptly to responsible health care provider. |
||
| 3. Once oxygen is applied, reassess your patient in 5 minutes to determine the effects on the body. | Hypoxia should be reduced or prevented. O2 levels should be between 92% and 98%.
Assess vital signs, respiratory and cardiovascular systems, and level of consciousness. Assess and implement additional treatments for hypoxia if appropriate. Reassess your patient if signs and symptoms of hypoxia return. |
||
| 4. If required, adjust O2 levels. | Changes in O2 percentages should be in 5% to 10% increments.
Patients should be reassessed (respiratory assessment including O2 saturations) after 5 minutes following any changes to oxygenation levels. Changes in litre flow should be in 1 to 2 L increments. Consider changing O2 delivery device if O2 saturation levels are not maintained in target range. Slow, laboured breathing is a sign of respiratory failure. |
||
| 5. If hypoxia continues, contact respiratory therapist or physician for further orders according to agency protocol. | Patient may require further interventions from the respiratory therapist or most responsible health care provider.
Signs and symptoms of respiratory deterioration include increased respiratory rate, increased requirement of supplemental oxygen, inability to maintain target saturation level, drowsiness, decrease in level of consciousness, headache, or tremors. |
||
| Data source: British Thoracic Society, 2008; Perry et al., 2014 | |||
Special considerations:
- The underlying condition causing hypoxia must be treated to manage and improve patient outcomes. For example, if hypoxia is caused by pneumonia, additional treatment for hypoxia may include antibiotics, increased fluid intake, oral suctioning, position changes, and deep breathing and coughing exercises.
- If a patient has COPD, check physician order for the amount of required oxygen and the expected saturation level. In general, COPD patients receive 1 to 2 L/min (Kane et al., 2013).
- Once oxygen saturation levels are within normal range, perform a respiratory assessment every two to four hours to monitor need for supplemental oxygen.
- When using oxygen therapy, assess the patient’s skin where the oxygen device comes into contact with the patient. The nose, chin, and ears may have skin breakdown due to the irritation of the tubing on the skin. Oxygen therapy tends to cause drying effects to the nares and mouth. To prevent the drying effect, consider increasing fluid intake (if not contraindicated). Perform frequent mouth care and apply humidification if the patient is receiving more than 4 L/min (Perry et al., 2014).
Critical Thinking Exercises
- A patient is admitted with COPD and pneumonia and has an oxygen saturation of 88% on 1 L/min of oxygen. Is this an appropriate oxygenation level for a patient with COPD? Why?
- A patient with no underlying respiratory disease is hypoxic with an oxygen saturation level of 91% on room air. What are four additional interventions that may help improve oxygen saturation levels without applying oxygen therapy?
